Considering all the excluded groups on the trial (page 3, kids, 55+, obese, weak immune system, a lot more), it's a lot of exclusions, how does one get from results on a study like this to declaring the vaccine safe for general use?
Generally speaking, experimental drug trials are run first on healthy groups and then in at-risk groups (old, young, those with co-morbidities). From the article, my guess is that they are expediting the sensitive groups trials, but unfortunately there's a lack of technical detail.
Source: My partner is an infectious disease specialist and we talk about this pretty much daily because I'm so curious.
But for this disease that's particularly bad because Covid has shown to be worst in 55+, obese, comorbidities, etc... which means that the trials on healthy groups are proving very little, since the virus itself is so much weaker on healthy groups.
>But for this disease that's particularly bad because...
Doesn't change the fact that, when you're developing a new drug, you want to test it in a way which will cause the least harm. You don't begin trials with those most at risk for obvious reasons. The primary goal of this phase it to asses the safety of the vaccine candidate.
I'm also unaware of any disease that isn't more threatening to people in relatively poor health.
"Spanish" flu was a notorious example: older people are believed to have had some amount of immunity from old strains, and the cytokine storms which made that strain so deadly are actually a consequence of having an active, robust immune system.
For much of 1918, a lot of people in their 20s getting the flu were also experiencing trench warfare, which can't be an optimal situation, both in terms of immediate self-care and co-occurring health conditions.
Older people were less vulnerable in the U.S. as well. The problem was that young healthy people were more likely to have an immune system overreaction. This applied to both genders.
You say it’s “obvious” but it’s the opposite of my intuition. Can you explain the logic a bit more?
I would have thought you’d give a risky new drug to the least healthy, most likely to die without it population, to raise the chance of survival from low to unknown.
Because you may not be raising it at all. The side effects could do more harm than the intended effects do good. So you need to do a large very controlled study with healthy people so you can more easily find side effects. Second, many side effects can be tolerated well by a healthy person but could be very dangerous in an at risk person. A drug that causes hypertension might not be a problem for a healthy person, but could kill someone with a heart condition. If you skipped this step, you could put people at risk of heart attacks and make it harder to detect the drugs effect on the heart vs already increased morbidity in those heart condition patients.
You are also evaluating the intended effects (as opposed to side effects), so you can see if it is actually doing what we want it to do, and how well. We could find out that the vaccine is very effective at preventing covid infections. But we could find out that it does not reduce the rate of covid infections, but does reduce the severity, or we could find out it does not reduce anything for reasons we don’t yet understand.
Once that is done, we will have a good understand of A. the level of benefit and B. the level of harm. From there we can make an educated decision to proceed or not. If we do, then it is approved and given to the general population, including those at risk. It is at this stage that the effects on at risk groups can be studied, during the ongoing monitoring of the approved drug.
Hopefully this answers your question and shows why this is the best way to do it.
There is always a balance of risks, and this is why there are ethics review board.
My intuition on this has become that the more certainty there is that you are to die without treatment, the easier it is to try relatively risky new treatments on you (with your consent). But say having stage IV pancreatic cancer is very different than having a comorbidity for a disease you haven't contracted yet.
Additionally with something like a vaccine, you are very interested in what it will do to the general population, not just the most vulnerable, because it should be rolled out to the general population. Anything screening program, you have to pay attention to the unlikely side effects since the denominator will be large.
Finally, you do these trials in phases because you need to find out if it is safe for humans first, then if it is effective.
Even among the 65+ survival is liable to be 90% even if infected and stand a good chance of avoiding the virus entirely even if they must wait a a few more months. Thus the probability of survival waiting isn't low to start with.
The proper calculation would be probability of infection * probability of death in the intervening months before we collect data on the efficacy of various options vs expected outcome if they just take the oxford vaccine now.
The users chance of survival is already quite high in the intervening period and while the benefits of the oxford vaccine are highly hypothetical they are also largely contingent on vaccinating everyone. People are liable to only see IF it works a 30% - 60% effectiveness, lower for some with worse immune systems. The real benefit is decreasing the spread of the virus until it dies out not merely the individuals benefit which will never happen if it turns out it doesn't work.
Worse it may be most apt to kill or harm those who are also most vulnerable to covid.
At worst the patient trades a very good chance of survival for a substantial downside with no upside and a future vaccination with a different vaccine they ought to have waited for.
There are a few factors -- one is that the major goal is to measure the side effects and safety of a particular new drug, in relative isolation... someone who is already sick is more likely to be on other drugs, thereby greatly increasing the risk of drug interactions.
Another is that when someone is already sick, they are more likely to not do well with any particular new drug (pretty much nothing is 100% effective for 100% of people), so you'd have to have some way to trying to discern whether the fact they got worse or even died is related to the new drug vs. just a natural progression. This can get complicated to measure.
And specifically for this particular thread, this is a vaccine, not a cure -- so in any case, when we say "least healthy" in this context, we're not talking about giving it to people who are already diagnosed with the virus, but rather to those who are _at most risk of complications_ from the virus, _if they were to contact it_. So it would be giving a drug to people who _don't_ immediately "need" it to survive, but who are still most at risk from any side effects.
You don't want people to drop dead from your experimental vaccine . As a general rule, the people least likely to drop dead from your experimental vaccine are young, fit, healthy people. Start with them. If they drop dead, well shoot. If they nearly drop dead, lucky you didn't start with the people who are one bad day away from the grave already.
In addition to what others said, if you know or suspect the procedure is extremely risky, and no other good options exist, you _do_ start with the least healthy.
As an example, the patient who got the first heart transplant:
“As a result of heart attacks in 1965, approximately only one third of his heart was still functioning. In late October, he went into a diabetic coma, but regained consciousness. […] He was also suffering from kidney and liver failure.”
It’s a vaccine, not a cure once you have it. So the people you would be testing it on wouldn’t be infected yet. Therefore you don’t first test it on unhealthy people when the vaccine might have unrelated nasty side effects.
You have a built in assumption in your statement that you haven't acknowledged: that the drug helps rather than harms. A new drug may help or it may harm.
If the drug turns out to harm people, a healthy person may be able to deal with it and recover. While a person that is barely hanging on to life may be pushed over the edge. There's no data to support a new drug raises the survival rate. It may in fact lower it from low to zero. During testing you generally want to kill as few people as possible.
Once more data has been collected on the drug, then the balance starts to shift toward giving it to at risk groups.
If you did start experiments with those most vulnerable you exposing them to far more risks.
Drug trials always start from learning more about safety of treatment (as opposed to efficacy) and once deemed statistically safe, you move to test for efficacy.
I assume you're thinking about treatments who could give a chance to those who have little hope/time for surviving. There's probably a chance they can benefit from taking experimental drugs but if we know little about it (because they are early in trial phases) we less confident this treatment will be useful and worst, we maybe not learn much from why it failed
Presumably the risks of an unknown response outweigh an as yet unknown benefit when testing is starting. These risks would be amplified for those with already compromised systems.
This is preventative medecine, as far as I know, most vaccines cannot be given to someone who already has the disease.
So it makes sense to target healthy people first, to test out the vaccine side effects, make sure there aren't many or bad ones, and then test out if the vaccine works. And then once you know it has low side effects and works, you can risk testing it on more compromised individuals.
One of the goals of pre trials is to establish that negative effects, if there are any, aren't caused by other factors other than the drug itself.
It's already hard to prove it on healthy candidates, it's pretty much impossible on candidates whose immune system is already weakened by previous conditions.
> I would have thought you’d give a risky new drug to the least healthy
Yes, but at this stage there is no drug. You're in the process of making the drug. And you don't want to test your beta versions on sensitive subjects.
Once nothing obviously bad happens, you can expand the test circle.
The high-risk population introduces statistical complications evaluating the results - were bad outcomes caused by the treatment under investigation or by the preexisting conditions?
But even if only healthy people get the vaccine, it could prevent the virus from spreading as much, thus protecting the people who cannot get the vaccine and saving countless lives.
As far as I know, they don't inject people in the trial with Covid, instead they wait long enough and use statistics to asses how many should have gotten Covid by now and if they didn't attribute it to the vaccine working.
Since healthy young people are more likely to get Covid, it might be this is the fastest avenue to knowing how effective the vaccine is.
But I am not a doctor or infectious disease expert or vaccine researcher.
There's a protective effect of 'herd immunity'. E.g., if we vaccinate all the ordinarily healthy people, then it should slow spread to better protect the at-risk groups. Sort of counter-intuitive, but it buys us time until we can figure out if this vaccine is safe for those groups.
Age and comorbidities (!!) always make a disease worse, obesity is a bit less common perhaps, but there's always something that's a risk factor, and the point is not to do something highly experimental and unknown starting with people who are already at increased risk.
What is the alternative? Skip testing it on healthier groups first? Imagine what would happen if the trial was going awry _with_ healthy people. You certainly wouldn't want to test this on vulnerable populations.
They prove that it is generally safe on a group less likely to throw spurious correlations at you ...because they are at risk Of just about everything not just covid
This phase I/II study's primary objective was to learn about the safety of the vaccine, and about whether it causes an immune response. I'm no expert, but I expect the phase III trials in the US and India will include a broader population.
Ah, thanks for clarifying that you participated in phase 1/2, I had not gotten this from skimming through the document, that makes a lot more sense to me. Thanks for sharing!
Not really qualified to answer this, but I would imagine follow-on rounds of testing. Also, those groups should be protected through herd immunity if everyone else gets the vaccine.
Vaccines often cause a minor cosmetic bump. If you see people with a triangle of bumps on their shoulder for example they have received a common vaccine for healthcare workers.
And the smallpox one can leave an even bigger scar. I suppose they don't want the liability for that which could impact the model's income
Maybe a stupid question, but do we need to vaccinate everyone? I remember reading that heard immunity is 70% or something - so could we get away with leaving the people out that it wasn’t tested on?
THEORY: Assuming 100% efficacy vaccine. In completely homogeneous population if people are randomly vaccinated the threshold where the diseases effective R drops below 1.0 is 1 - 1/R. For example if R = 3.0 you need to vaccinate 66% population until infections start to decline.
REALITY: Assuming 75-90% efficacy vaccine, vaccination is non-random and population is heterogeneous. You want to vaccinate everyone who agrees to take it. Just like with children diseases, there will be clusters of anti-vaxxers, or people just don't bother and they are often clumped together, travel around the world and spread the disease.
It's not a stupid question, and I've heard that some vaccines are aiming to be approved only for adults at first. This would make sense not only because, as you say, you can start to approach herd immunity without vaccinating everyone, but also because children are weaker spreaders.
Obviously "herd immunity" is more of a gradient than a cut-off, and it's much easier to approach it if we can vaccinate everyone, but we can definitely speed up the process (including the months-long process to even get the vaccines to everyone) if we can start vaccinating some people early.
Theoretically the % of people needed to reach herd immunity is a function of how infectious the virus is. They use a number R to represent for each person who gets infected how many people they go on to infect. This changes over time as different measures come into place like lockdowns, masks, and social distancing. The basic reproductive number R0 (R-naught) is how infectious the virus is initially without any of those measures in place. The formula for the % of people needed to reach herd immunity is R0-1/R0. So if R0 is 4 then you need 3/4 of the population. If R0 is 3 then you need 2/3.
The vaccine may itself not be perfectly protective, and the herd immunity threshold only works if the people vaccinated are random. Otherwise any unvaccinated population can have an outbreak.
You should be able to see that Covid-19 is in fact a disease listed in the table on the wikipedia page you reference. You should also be able to see that the percentage required for herd immunity effect to begin (the 'herd immunity threshold') is a function of the R0 level for each disease.
In addition, to question of "can anyone really say for covid-19", I suppose the answer is 'No, but I would trust that the consensus of the scientific community of infectious disease experts is the best estimation we can get.'
i haven't read through all the questions asked here, but yours is perhaps the least stupid
i suspect you may already know the answer to your question; of course not everyone needs to be vaccinated - that's the job of any reasonably healthy immune system and this virus, which has not been properly isolated by the way, and that comes directly from the CDC, is not particularly dangerous, and that comes directly from the WHO
any thinking human being knows that masks are, at best, largely ineffective at preventing transmission, as is "social distancing" - the way governments are handling this "pandemic", which by definition is not a pandemic, is killing far more people and ruining far more lives that the virus ever will
the question then becomes, why? why are we being asked, and compelled in many case, to wear ineffective masks? why are being threatened and arrested in some cases for not distancing when there is no creditable scientific evidence to support that distancing works?
furthermore, the rt-PCR "test" that is used by many labs to diagnose COVID-19 is not a test - it is a procedure designed to amplify a tiny amount of RNA or DNA - it was never designed to test for this or any other virus and it does not produce a binary result, so in the end , we have NO idea how many cases there are, and it gets worse than that because apparently PCR is looking for any corona virus, alive or dead! that means that anyone that's ever had a cold can test positive (along with people that died in motorcycle accidents, fallen down stairs, or got shot in the face apparently)
the number of 'cases' is meaningless and the survival rate is exceedingly high, and if we make an adjustment for the radically inflated number of deaths, it becomes very questionable whether there even is a "novel" corona virus or whether it's the flu
lastly, even if one is not reasonably healthy, or just doesn't wish to spend a lot of time being sick, all that required is high-dose vitamin C along with D3 (and zinc wouldn't hurt) - what's a high dosage? 4 grams+ / hr. for an adult, not that it's critical because no one has ever died from vitamins (minerals is a different story)
> this "pandemic", which by definition is not a pandemic
> any thinking human being knows that masks are, at best, largely ineffective at preventing transmission, as is "social distancing"
> it becomes very questionable whether there even is a "novel" corona virus or whether it's the flu
You know, I live in Adelaide, where we haven't had a single locally-acquired case in several months. I've been wondering how almost every other city on the planet has been screwing things up so badly when we've not really done all that much apart from having a quick reaction and social distancing appropriately.
My question is now answered: those cities have people like you, willing to spout even the most blatantly abject conspiratorial nonsense for the sake of advertising your own website.
Please show some responsibility for the lives of those around you.
As someone living in Melbourne it's been frustrating to see this same nonsense spread locally by a very vocal minority, followed by "lockdowns don't work".
I'm celebrating that following the science here has taken us from > 700 new cases per day, to our second consecutive day of zero (and lockdown ending less than 3 hours from now)
The control group will not be given the vaccine, but a placebo.
Clinical trials are phased. Typically you start with a very small group of people to evaluate toxicity (e.g. below treatment levels of a drug), then a slightly larger group looking for side effect, then a significantly larger group looking for desired effects, and finally a broad group looking for safety and efficacy.
That phase 3 study for the Oxford vaccine is already underway, and its initial findings are what the article is referring to. It was one of the first (possibly the first, I'm not entirely sure) to enter phase 3.
Extrapolation. Is there a scientific rationale as to why the vaccine would NOT be safe and effective in a new population? If not, approve it for that population. If there is rationale why it wouldn’t be, ask for more data.
Noise in the data - you want as clean a population as you can get. If you start including people with chronic conditions, as soon as someone in your trial dies you get to play a game called "prove that it wasn't the vaccine that killed them".
Same with people over 55 years old - they are known to respond differently to vaccines. The worst thing in the world would be showing a 49.4% reduction in Covid infection rate (the FDA wants 50% minimum) and then being forced to do a bunch of handwaving about how your results were skewed by the 55+ patients in your study and "by gosh, I swear it would be over 50% if we adjust for them using this methodology we just made up". Nobody will believe you and you'll be relegated to "that vaccine that almost works".
Ethics - Kids aren't (well, very rarely) dying from Covid, but they could die after getting your experimental vaccine. Kids sickened by experimental drugs makes for bad press, not only you, but also the FDA. Easier to just exclude them for now.
I'm surprised they don't seem to do frequent and regular COVID testing of participants to catch asymptomatic infections. Naively, it would seem worthwhile in order to predict how well the vaccine would slow down the spread.
I guess the reason is that the study is narrowly tailored to vaccine approval requirements?
The study is tailored to the standards of vaccine approval, of course it is. They need to prove safety and efficacy, so they design a trial which will allow those factors to be measured.
Kind of difficult to prove efficacy if you don't know how many people in your trial were infected with the disease you're trying to vaccinate against though. But do bear in mind as mentioned in other comments this participant was not in the phase 3 trial, and phase 3 is where the immunity given by a vaccine is tested. Phase 1 and phase 2 are much more constrained studies intended to determine if it's safe to give the vaccine to enough people to evaluate immunity.
Since this is would presumably be testing for efficacy I guess they would have a number of pre-determined "interim analysis" points in the study when X count of people report becoming positive for the coronavirus. If the proportion infected in the treatment vs control is too high (i.e. lots of vaccinated ppl got sick) they will stop the trial and consider the vaccine a failure. If too few get it, they might stop the trial and immediately move to a Phase III study to confirm their result - that is they accelerate the trial to get the treatment out quicker.
I am unsure if they will have some lower bound for acceleration for this vaccine, since the downsides might not be apparent for a long time.
More than 300000 people a day get tested for coronavirus in the UK according to [1], and the testing capacity is even greater than that. This is enough to cover study participants.
I would imagine that volunteers would also be willing to get tested, though perhaps the worry is that such a requirement might cause more of them to drop out of the study.
>You will be compensated for your time, the inconvenience of having blood tests and procedures, and
your travel expenses. The total amount compensated will be approximately £235 - £625 depending on
the exact number of visits and whether any repeat or additional visits are necessary.
To add some context to this, medical trials generally only compensate time (at a low hourly rate) and expenses, occasionally increased slightly to compensate for hardship.
They deliberately do not pay large amounts, because the money is not supposed to overly-incentivize the participation, to avoid ethical issues where someone might choose to participate in something very unsafe only because the reward seems so large.
I did various medial trials in college for money and have mixed feelings about this. When sitting in the various waiting rooms, it was very clear that was only one kind of person that did "open" (not targeting people with a disorder but rather recruiting healthy volunteers) medical trials: the poor. I got to know lots of of people well (we were frequent flyers in the medical trial world), and our common characteristic was that we really needed the money.
It's kind of like non-pay electoral offices. You only get candidates that can afford not to work. In medical trials, you get the kind of people that are willing to, for example, get infected with the common cold and have you blood drawn 6x a day for 4 days for about 80 bucks a day. It was not horrible, but often uncomfortable. Study recruiters still call me, and now that I have a decent paying job there is no way I would ever consider doing those kinds of studies again. Simply not worth it.
The problem is increasing the reward makes the people “who need the money” much more willing to engage in trials with much worse possible side effects. As long as the pay isn’t life altering money for anyone, nobody will volunteer to do something with a high probability of life altering side effects.
The treatment itself is also free. For a vaccine trial that's not much of an incentive, but for things like cancer trials it can be extremely valuable.
>Until now, this vaccine has only been tested on laboratory mice and other animal species and this is
the first time that the vaccine will be given to humans.
This is only one of 11 vaccines now in phase III efficacy tests.[1] Six vaccines already have "partial approval", but those are the ones in Russia and China, which may or may not be working, and the governments decided to try anyway. All of those provoke an immune response. Whether it's enough of the right immune response is found out in phase III testing.
Something is probably going to work. The big question is how well. A 50% effective vaccine might be an overall lose - only half are protected but more than that abandon masks and social distancing.
The Johnson and Johnson vaccine, if it works, is the easiest to use of the early leaders. One dose, and it doesn't need to be refrigerated to dry-ice temperatures like some of the others. The Merck/IAVI vaccine is only in phase I, but it's a pill. If that works and is highly effective, it will be possible to wipe the virus out worldwide in a second round of immunizations.
> A 50% effective vaccine might be an overall lose - only half are protected but more than that abandon masks and social distancing.
I remember a similar argument being used against face masks. (That they are not perfect, and may cause harm by giving false sense of security.) Perhaps we should be more careful about perfect being the enemy of good.
The availability of masks is far higher than vaccines, though. You can order a box of masks on the internet and have them same-day delivered to your home. The scarcity and logistics of delivering a vaccine once it becomes available are both factors that make the effectiveness that much more important.
Not happening, recent polls suggest that in Germany, 55% percent of the population is willing to get the vaccine.
That isn't enough for herd immunity (at around 60%) and real vaccination rate will be even lower.
There is also no chance in hell that Germans will allow a government-mandated vaccine. It's unconstitutional and there is heavy opposition to government-mandated anything throughout all of society.
So we will be stuck with this virus. But you're free to get the vaccine yourself for your own protection.
Well, the rest will become immune the natural way fairly quickly: By contracting the virus.
Once a vaccine is available and a large share of the population either has been vaccinated or has the opportunity to be vaccinated maintaining the current measures can't be justified anymore.
Nooooooo - how are people still saying this. There is little evidence at this stage that immunity can be gained in this way, for this particular virus.
There absolutely is evidence of this. It's just not "immunity for life", which is what people commonly seem to think of when they're talking about immunity.
When you've had an infection with one of those rather harmless yet still pesky other coronaviruses - otherwise known as the common cold - you're also immune, for a limited period of time, that is.
There are plenty of cases of people being reinfected quite quickly and frequency of exposure also seems to correlate with serious illness ... the science is still very much “out” on this.
“We conclude that neutralizing antibodies are stably produced for at least 5-7 months after SARS-CoV-2 infection,” the team of researchers, lead by Deepta Bhattacharya, an immunobiologist at the University of Arizona College of Medicine, wrote in their report."
Interesting. This research is apparently just a few weeks old. I look forward to seeing it corroborated and replicated!
EDIT no mention of it in Nature's covid roundup [0]. They must be censoring the research. I've tried googling the author and he seems to be some form of contrarian.
It seems likely that percentage will increase as more people are vaccinated and do not have adverse side effects, so people gain trust in the vaccine.
The same is true for other vaccines. See for example [the figure on this page](https://www.gavi.org/vaccineswork/qa-ola-rosling-gapminder): in this survey, in Germany, 13% said they believe vaccines are not safe in general, but only 3% of babies are not getting the measles vaccination.
So let's hope many of the people that currently are not planning to get the vaccine, will change their mind and actually do so in the end. I think good information campaigns in the media and testimonies of friends that have received the vaccine will do a lot to mitigate this problem.
At a considerable cost. There's a large number of people for whom the vaccine won't work when it has been taken correctly or who cannot take the vaccine because it will react very badly with their chemotherapy or whatever.
This "let Darwin deal with the anti-vaxers" solution, though initially attractive, ends up being sociopathic when you dig into it.
I'm not saying it is attractive. Just that that will be the consequence, it is not sociopathic on my end, it is on theirs. By not taking the vaccine they are also risking the lives of others who do take it and for whom it isn't effective or who can't take it.
What percentage of the population needs to be vulnerable for the entire population to be forcibly inconvenienced for their needs? When is it the responsibility of the vulnerable to protect themselves vs forcing society at large to protect the vulnerable? Certainly there is some threshold, considering that we didn't shut down society in the past for the tiny percentage of bubbleboys with no immune system. To call people sociopathic is to close your mind and not see the real gray areas. So to ask again, what percentage of society needs to be vulnerable in order for it to be ethical to coerce everyone to do something?
> Certainly there is some threshold, considering that we didn't shut down society in the past for the tiny percentage of bubbleboys with no immune system.
Well, thankfully we haven't done this today either. This virus appears to affect more than just those that die from it, and that group of victims already includes more than a "tiny percentage of bubbleboys."
The virus kills on the order of 1% of people who contract it, and can cause serious illness or death even for healthy people, so anyone who is able to get the vaccine should get the vaccine. It's not like you're being asked to give up an organ or something; you're being asked to protect yourself, and protect those unfortunate enough not to be able to get the vaccine themselves as well. Rather than quibbling over percentages, why not ask yourself what ethical foundation a healthy person could have to not get the vaccine once it's been proven safe and effective.
The alternative is to make vaccination a precondition for a lot of government services, particularly public education. Also there needs to be a heavy advertising campaign advocating for vaccination.
No, but neither is that an issue of bodily autonomy.
Bodily autonomy is about being in control of what happens to your body — it does not mean you have carte blanche to do whatever you want with your body.
So, logically the solution is not to mandate the vaccine, but to restrict what unvaccinated people can do, where necessary to protect others. For example, if not vaccinated, you should continue to wear a mask while indoors in public (as long as local virus cases are above a given threshold), as well as avoiding large gatherings.
That's clearly no choice at all. It either is a choice or it is not, and restrictions that severe clearly indicate that no, it would not be a choice. You realise how transparent that is, right?
Masks and social distancing are not sustainable forever. A lot of people are going to abandon them regardless of whether a vaccine is available, so any safe vaccine would be a win even if effectiveness is low. Seasonal influenza vaccines are sometimes as little as 20% effective when the circulating strains don't match predictions, but even 20% is a lot better than nothing.
To us in Brazil, this vaccine is particularly interesting because not only is it one of the vaccines being tested here (together with FIOCRUZ in Rio de Janeiro; another one is Coronavac from Sinovac together with Instituto Butantan in São Paulo), but also there's already an agreement to manufacture it in the country (https://portal.fiocruz.br/noticia/fiocruz-assina-contrato-de...).
Can someone explain to me why double blind is necessary or useful for a vaccine trial such as this? It seems obvious to me on something like a pain medicine, but on a vaccine it seem a pointless. Is placebo an actual issue with a vaccine?
It honestly seems borderline unethical to give people a placebo vaccine.
Also, there is a very strong risk, given the global situation, that the longer placebo-controlled trials go on, the less reliable the data will be, because control-group subjects will ignore the rules of the study and go get vaccinated as soon as it's broadly available just in case. So even just looking at data quality and excluding other considerations, placebos have major risks that probably outweigh the benefits of administering them for months or years like a usual vaccine trial would.
People who know they've been vaccinated will behave more recklessly than people who haven't been vaccinated. You need to have a control group, in order to assess the efficacy (and safety) of the vaccine. If the control group is wearing masks and socially distancing, but the vaccinated group is going partying at bars and clubs every night, then comparisons of how often each group gets infected won't have much meaning.
It's only unethical to withhold the vaccine if you know that it's safe and effective. The whole point of the study is to figure out if that's the case. It's possible for vaccine candidates to be ineffective, or even harmful (e.g., antibody-dependent enhancement).
What you’re describing as “reckless behavior” is just normal behavior in a non-covid world. If vaccine candidates are social distancing, wearing masks, and staying home how will the researchers get the data they need? If you are following “covid best practices” it is extremely unlikely that you will contract covid. Would the researchers not want people to go out and live their normal lives?
The point is if the two groups behave differently wrt risk then the trial is probably ruined. Maybe you're assuming the vaccine will be 100% effective; experts I've heard are saying to expect something like the flu shot.
Experts need to control to control expections. The flu shot like 50% effenceny is a possibility, and we know anti vaxxers latch onto that with confused statistics. The flu shot is poorly effective because the flu mutates though, covid is more stable so odds are that the vaccine will be more effective, but we are still playing odds of something we don't know, so it is best to assume the worse.
The flu vaccine is more effective at preventing serious disease than it is at preventing infection. Even a vaccine that only prevents you from getting seriously ill can be incredibly useful.
The inactivated polio vaccine, for example, does not prevent infection. It just prevents disease. That means that it cannot confer herd immunity (vaccinated people can act as asymptomatic carriers, leaving unvaccinated people at risk), but for most people who are vaccinated, it eliminates the most serious consequence of polio infection - paralysis. The SARS-CoV-2 vaccines might end up being the same, conferring protection from disease but not from infection, and even that would be important.
Well in this scenario I am suggesting that a placebo is a waste of time and we don't need two groups. I am not assuming the vaccine will be 100% effective, or even effective at all. But in order to get meaningful data you can't have all your participants taking the most extreme precautions. The vast majority of American citizens have not, and will not, get Covid.
A few percent of Americans have been infected with SARS-CoV-2. In a study of 30,000 people, enough people will get infected within a few months to give good statistics. At the current rate of confirmed cases in the US, you'd expect about 10 people in the study to get infected each day (fewer if half of them are vaccinated and the vaccine works).
Without a placebo group, how will you measure effectiveness and safety? You need to monitor a statistically equivalent group of people to determine the difference in rates of infection and disease, and to look for side-effects.
You need both groups to behave in the same way. Phase III trials are enrolling enough people (tens of thousands) so that a sizeable number will likely contract the virus within a few months. They specifically run these trials in places where the virus is spreading (this is why Chinese vaccines are being tested outside China, in places like Brazil).
> Would the researchers not want people to go out and live their normal lives?
That would be great for the trials (assuming both the vaccinated and placebo groups behaved identically). But most people would consider it unethical for researchers to encourage the trial participants to increase their likelihood of exposure to the virus. People who sign up for vaccine trials are not signing up to get CoVID-19.
> If you are following “covid best practices” it is extremely unlikely that you will contract covid.
It’s spreading like wildfire to people following best practices too all over the world. It only takes a small subset not following these practices to spread it all over.
If you tell people whether they're now vaccinated, they're going to take a lot more risks.
You may still have increased risk taking behavior if you don't tell them whether they got the real vaccine or placebo, but it will be equally increased across the experiment and control groups.
It's rudimentary to figure out if you got a vaccine or placebo. Live vaccines tend to produce the type of temporary localized soreness you experience with a flue shot. Placebos do not.
Really it's about measuring how likely vaccinated participants are to contracting the virus than those that received the placebo.
A real vaccine, with side effects that are similar to what is expected of the covid-19 vaccine. It is a well tested and safe vaccine and it will protect you from meningitis but not from covid-19.
They are doing that exactly for the reason you are mentioning. Of course, participants are aware of the nature of the placebo they might receive.
A placebo doesn't have therapeutic value but it doesn't mean it has no effect at all. And the Meningitis vaccine doesn't have therapeutic value in the contest of Covid-19.
In fact, there are even placebo surgeries. They put you to sleep, cut you open, and stitch you back without actually doing anything inside your body. It is far from nothing, the anesthesia and the incision are real. It is important because you want to compare the effect of the actual operation to everything else that is involved in a surgical procedure.
Having them expose themselves more to the virus is a "good thing" (though tell them how long should they wait for the immunity to set in)
Yes, with the control group you would have a base for how many people you would have expected to be infected, so there's that, but you "could" get that from other observations
> Yes, with the control group you would have a base for how many people you would have expected to be infected, so there's that, but you "could" get that from other observations.
Getting this number for a distribution of people as similar as possible to the people in the experimental group is, in fact, the primary purpose of having a control group. There is no better way to predict this number, as you can't predict how likely a particular person is to catch coronavirus at a particular time, in a particular location.
You also need a control group to get the number of various medical problems expected in the experimental group, even if the vaccine doesn't cause them. This also depends on time, place, and behavior.
So, if you create a reason for people in the control group to behave differently from experimental group, for instance by letting people find out which group they are in, you defeat the purpose of having a control group.
I'm not denying there's the need for a baseline to compare to, but the need to have an dedicated designated group to be the 'official control'. I agree it makes things easier statistically.
> So, if you create a reason for people in the control group to behave differently from experimental group
Yes and here lies a minor catch, both those groups might behave differently from the population in general (even though they aren't "supposed to")
>Why are so many people commenting when they clearly don't understand knowledge-creation/statistics/methodology?
Because (a) we want to understand. and (b) reasonable experts differ on what constitutes proper methodology which is constantly being improved.
Surely the effect size of a useful vaccine is large enough that modified behaviour of the vaccinated does not matter at all. We're not looking for a small incremental improvement in contraction rate of the virus here, we're looking for a very large percentage of those who have been administered the vaccine not getting covid. Yeah it could change behaviour but so what? How is that going to bias the result to suggest it isn't working if it is? (or vice-versa)
Anti-scientific sentiment is at high levels because you don't get someone to personally explain basic statistical concepts that you could have googled yourself?
To add to the other comments: because giving a placebo is essential for the experimental results to have any validity, not giving a placebo would be imo way more unethical, since it would mean you are exposing people to a medical risk (experimental vaccine) for no scientific benefit.
(Needless to say, running an invalid vaccine trial also has very bad consequences: it would delay the actual deployment of a working vaccine to the general public, resulting in millions of unnecessary person-hours of potential virus exposure.)
Are they testing for side effects in all three stages? I thought the first two trials were for safety and the third was for efficacy. Is that incorrect?
I imagine: If a given side-effect occurs at the same rate in both groups, it's unlikely to be caused by the vaccine and is more likely to be psychosomatic.
Data on adverse reactions is captured by the CDC/FDA/HHS throughout the lifecycle of the vaccine, from all the phases of clinical trials to its use in the general population. Its required by law.
I'm in the trial. It's really exciting, not least because form a purely selfish point of view, I might be immune already! ...or not. But it's exciting either way!
Have you experienced any side effects, even mild like injection pain or fatigue? I'm in the Moderna study and feel pretty disappointed that I may have gotten the placebo.
… or you might have been lucky with getting minimal side effects.
Double blinded placebo controls are critical to clinical trials so you shouldn’t be disappointed one way or the other. Even if you are in the control group you’ll have the opportunity to get the vaccine after you’ve helped prove its efficacy and safety.
That’s actually a big concern. The FDA will likely approve based on an interim readout of data. However, they will want the full set of data around safety and efficacy.
But what happens if a vaccine gets approved while you’re in a trial and not sure if you got the placebo? Well, you can drop out and just get the approved vaccine.
Of course that will trash the original trial you were in.
Did they disclose what the control group got as a placebo? For instance, in this study it's a meningitis vaccine, so it could still have those side-effects if you've never had that vaccine.
Not OP but from the reports I have read, people who have been given placebos will be informed if the actual vaccine is found be really effective. This is for ethical concerns (in the sense that it would be unethical to not vaccinate people who have got a placebo if the real vaccine is really effective)
For some history on the matter of ethics in medical research, the 'Tuskegee Experiments' was among the most infamous biomedical research study in U.S. history [0].
Yes. I had generalized pain in both arms after the first injection. Not the second. Nothing worse than you'd expect from another vaccination.
Mild fever for 48 hours that meant I was too tired to exercise, but I was more than fine to work. (I'm a software engineer. I think if I had a more manual job, I would've struggled!)
My follow-ups are every 2 months at a local hospital. They take general observations, ask about side effects and take a small blood sample (presumably to test for antibodies)
Do you know if the placebo is laced with something to simulate those side effects? Or is that a clue that you got the real thing? Also I'd assume the vaccine would make you test positive for the immunological screening tests?
This trial doesn't use a placebo, it uses an active control. In this case, an already licenced vaccine for meningitis.
So the side-effects I had could be due to that vaccine, I don't know.
Yes, in theory it would make me test positive for an antigen test. So I'm barred from donating blood as my sample would show as positive for COVID-19 antibodies.
Wow, if they're insisting on COVID-19-antibody-free blood for donations that's going to cause problems as a greater percentage of the population gains antibodies to it. I guess they'll have to change to a specific test for current infection.
This is a rule only for those in the trial. If I donate blood today, having had the vaccine, and the blood donation service checks my blood for antibodies and informs me that I had COVID-19 (or so they think!), then I will have been unblinded in the trial which isn't allowed.
This isn't the case for the general population. I'm also not allowed to take part in any other antibody tests that might accidentally unblind me in the trial.
I'm receiving no money for my participation. I wasn't in the initial Phase I trial, a few hundred people had already received the vaccine before me with no unexpected side effects.
I guess I'm risking it because someone has to. Vaccine trials are incredibly safe and highly regulated. In reality, the worst-case was that it didn't work rather than my head exploding.
I have a "red alert" card so if I'm found unconscious a paramedic knows to contact the study team to find out if I'm in the control arm or I've had the active vaccine so they can rule out if it's important to why I was found unconscious!
But it is just a piece of paper that the team printed out, and I think I lost it.
It's in my iPhone medical ID which I carry round far more often than my wallet. (Paramedics almost always check that here in the UK)
The likelihood of it being of diagnostic usage is pretty low anyway. A vaccine is highly unlikely to cause the sort of reaction that means I won't be conscious.
It's worth pointing out that during a pandemic, while participating in a trial does carry a risk, so does not participating. A participant has some substantially greater probability* than the general population of avoiding an infection which apparently carries a risk of death or long term debilitating effects.
* You'll have to incorporate the probability of being in the control group, of course, but the overall probability is still significant.
>It's worth pointing out that during a pandemic, while participating in a trial does carry a risk, so does not participating. A participant has some substantially greater probability* than the general population of avoiding an infection which apparently carries a risk of death or long term debilitating effects.
Participating also carries risks beyond simply that of the vaccine. Being exposed to any kind of healthcare setting is extremely dangerous right now. I'm taking part in the Moderna trial, and honestly I'm considering dropping out before the second injection. The risk of going into a clinic multiple times where I hear people coughing all over the place is starting to seem unacceptable to me given that I'm fairly certain I've been given the placebo.
FTR, most side effects appear (according to what Moderna published so far) only after the booster shot. So IMO you can't tell yet if you were given the vaccine or not.
Oh yeah, that's for sure. The idea that there's a pretty decent chance that I've been vaccinated already which means I don't have to wait for a vaccine is great.
My life can begin to go back to normal potentially months before it otherwise would.
I'd assume that one would be socializing with the same groups of friends/family that they had pre-COVID. With that in mind, wouldn't OP have already established a foundation of trust within those groups? Maybe this sounds naive, but why have friends if they're not capable of trusting you?
There's a surprising number of comments about people trusting me.
It's interesting because that's, not once, ever been a concern. If people don't want to spend time with me until vaccination is more widespread, then that's fine. But the intersection between those who don't trust that I've been vaccinated and those who don't trust vaccination anyway is probably pretty large...
It's worth remembering that Phase 3 trials follow Phase 1/2 trials, and those earlier trials are responsible for assessing the general safety of the vaccine. Phase 3 helps assess safety concerns among a much larger and more diverse group of people, but it is primarily about proving efficacy. They don't give out tens of thousands of vaccines (Phase 3) without a lot of data already showing the vaccine is safe.
By the time human trials commence, we're as sure as we can be that it's safe. Due to how the system is set up at the governmental level, whenever any participant in the trial experiences adverse reactions, the trial is halted, until an explanation can be given. It's a serious concern that can and does lead to products not being approved by the FDA. Not being approved = loss of tens or sometimes hundreds of millions of dollars. People take this stuff very very very seriously :)
What if something goes horribly normally and you catch the virus the vaccine is supposed to prevent?
It's a risk tradeoff, different between the phases. I'd probably volunteer for a phase 3 trial if one was available in my area. Phase 1 would be a bit too hot for me.
I wasn't interested in Phase I. My trial is Phase II/III. I was by no means the first to be vaccinated. Any major, common, reactions had already been pretty safely discounted.
A quick summary of were the Oxford vaccine stands since it's hard to follow:
- When will the vaccine be ready?
After the Phase 3 efficacy data is reported, assuming that the data shows that the vaccine prevents COVID or reduces COVID severity. This happens after enough people in the trial get sick with COVID. Then they unblind the groups and see if the people who got sick were in the control group or the vaccinated group. Essentially we are all waiting for a few 10s of people to get COVID. You can guess that the UK, South Africa and Brazil trials are getting very close to this since those trials have been running for months, but the US trial has recently started and is being run separately and wouldn't be very close yet. So the UK would probably have the first chance of approving this vaccine.
- What do we know about vaccine effectiveness so far?
So far, they've published initial safety data and immune response data in both healthy young adults and now in older adults. That all looks good - basically, the vaccine generates a lot of antibodies in everyone who takes it. So in theory, it should work. Separately, other groups have done testing to verify that the vaccine is operating the way it should at a biological level. There were also very early animal tests to show that the vaccine reduced the severity of COVID and prevented serve lung symptoms. In those tests, the vaccine didn't totally prevent transmission, but the animals were injected with a large amount of virus and it's not clear how humans will react in the real world (hence the wait for Phase 3 trail results).
- If it works, how long would immunity last?
No one knows until we wait and find out. But people vaccinated with the experimental SARS-1 vaccine still show antibodies over 10 years later, so the hope is that it could be long lasting.
- Didn't they have to stop this trial at one point because someone got sick?
Actually, at least 3 adverse events have occurred. Early on, one person got symptoms consistent with typical vaccine side effects, but it was determined that the person had a previously undiagnosed, unrelated disease. Second, there was the highly publicized case where a patient suffered temporary spinal inflammation and recovered shortly. It is unclear if this event is related to the vaccine, but trials in all countries have resumed so the various government agencies seem satisfied. Third, a patient in Brazil died of COVID but it was reported that the patient was in the control group and hadn't received the vaccine. Very little information from these cases is reported because of health privacy laws, so some of this information comes from media reports as opposed to official announcements. None of it seems inconsistent with a normal vaccine trial.
- Would you feel comfortable taking it yourself?
Yes, I did (I'm in the trial). No side effects worse than a flu shot personally.
> I'm assuming you also don't know if you got the active substance or a placebo?
Yep. In the UK, they used an existing, unrelated vaccine with similar side effects as the control so it wasn't obvious which one you got. In some countries and for some of the other vaccine trials, they are just using saline as the control so it seems like a lot of those people would know.
You ever gotten a flu shot? Usually your arm hurts for a day or two after, even if there are no other symptoms. This is a side effect of the immune response, as your body fights the "infection" at the point of injection.
And here I've thought the sore arm was your body reacting to a hypodermic needle going into your upper arm muscles. I suppose it could be a little of both though?
I don't get any difference, though I do always get warned about this (I qualify for a free flu jab every year because part of my immune system had cancer when was I was younger)
This year I actually had a moment as I was preparing for bed that night when I went "Oh shit what's this?" because I felt a bump that hadn't been there before on one arm. It was the tiny sticking plaster the nurse applied after the injection to cover the site. That was the first time since leaving the clinic I'd even remembered I got a jab that day. I peeled it off, put it in the waste and went to bed.
A lot of the things that happen are psychosomatic, so those would happen even if it was saline (or, I suppose they might not happen if you believe it was just saline even if it was really the active vaccine) but there are effects above this baseline in some people some of the time.
>Early on, one person got symptoms consistent with typical vaccine side effects, but it was determined that the person had a previously undiagnosed, unrelated disease. Second, there was the highly publicized case where a patient suffered temporary spinal inflammation and recovered shortly. It is unclear if this event is related to the vaccine, ...
This seems rather worrying as these Phase 1 and Phase 2 trials are pretty small, no? What are the odds these patients got this from the vaccine vs whatever else they had going on?
I just can't shake the fact that this particular vaccine seems to have some safety issues. We'll see in Phase 3 if this shakes out, but I would like to understand why governments feel safe about these developments.
This is exactly the kind of question the trials are designed to answer, yes. We know roughly the background incidence rate of diseases, so you can expect some percentage of participants will be affected by those diseases. It's also important to remember your basic statistics fallacies: the question is not, what are the odds that any of our participants come down with MS, which is a very tiny chance. The question is, what are the odds that any of our participants will come down with _any_ background disease, which is a much larger chance. It is very likely to happen, and indeed it does. They still pause the study to run the numbers and make sure the new diagnoses are not outliers from the background rate.
Out of hundreds people picked random, it's not unlikely someone will have some undiagnosed health problem. People get diagnosed with new diseases all the time.
That's right. Out of ~18,000 people total across 3 countries (UK, South Africa and Brazil), there have been 3 reported events requiring a pause, of which two involved people who got the real vaccine and one who got the placebo.
Keep in mind they pause anytime anything serious happens to anyone in the trial to give them time to make sure the vaccine didn't cause it. Pauses are a good thing - they are a sign they are following the protocols and not just pushing something through.
The most interesting part to me is that we require some people to get sick. Which totally makes sense. But what if the vaccine happens to be 100% effective? Do we ever get to end the trial?
yes because people in the control group would get sick. Once a certain amount of people get sick they see how many of those people were in control vs vaccine group. In your hypothetical, 100% of the sick people would be from the control group.
Well, it's still good news, but an injected vaccine may not lead to sterilizing immunity - i.e. vaccinated persons might still be able to transmit the disease:
> Without a strong mucosal response, injected vaccines may be less likely to produce so-called sterilizing immunity, a phenomenon in which a pathogen is purged from the body before it’s able to infect cells, Dr. Durbin said. Vaccinated people might be protected from severe disease, but could still be infected, experience mild symptoms and occasionally pass small quantities of the germ onto others.
Even so, reducing the severity would be great. Even if a patient doesn't die, Covid-19 can have devastating and long-lasting effects. If a vaccine could reduce it to just a mild flu, I think that's good enough. You just have to inject everyone and probably add it to the standard child vaccination set.
Articles like this: https://www.news-medical.net/news/20201026/COVID-19-now-like... make me think that's seriously unlikely. I mean unless, you are talking about one of the historical flu pandemics. Yes, this is less deadly then the 1918 flu was in 1918. Then again, I think the 1918 flu would also be less deadly then it was in 1918 if it occurred for the first time today because of other medical advancements.
Because it's substantially more deadly than the flu. (That's not counting the survivors who suffer permanent organ damage.) Please update your facts before posting in public on this topic again. I suggest sources other than Fox News.
If you're about repost right-wing canards about how it's less deadly for children, please review salient facts about infectious diseases, such as the fact that they are infectious. The goal of vaccinating younger people is to protect those whom they might infect.
There's never been any belief among the scientific community that any of the vaccine candidates would provide sterilizing immunity. That was just a pipe dream.
It seems that COVID-19 is often passed at superspreading events. If the vaccine could nevertheless prevent people from superspreading then it might still have a substantial effect.
Though, sometimes people think vaccines just prevent someone getting a disease. Stop it completely in its tracks. That's true for some, but it's not that simple for others.
Unfortunately a measured immune response does not ensure:
- That the virus can't be transmitted to others
- That you are less likely to catch and replicate the virus
- That you can't get ill from the virus
- That you can't get "long covid" symptoms
- That you can't die from covid
- That the immune response lasts for more than a few months (this is why we keep getting some of the same cold viruses; our immunity to them doesn't last)
- That the R number goes down (if it doesn't prevent transmission)
- That the R number doesn't go up (if people change behaviour in response to knowing they or other are vaccinated)
- That the virus won't evolve a workaround in response, like the rapidly mutating flu viruses
An immune response certainly suggests those things. But we can't be certain from immune response alone. Consequences need to be measured as well. We'll have a real solution when those sorts of things can be demonstrated, but it will take much longer to find out unfortunately. Probably we have to deploy a vaccine on a large scale somewhere before we can even find out how effective it is in the ways that ultimately matter.
Still, if a vaccine combined with uptake and people's behaviour reduces R below 1.0 at scale, that's enough to be a breakthrough. The greater the reduction the better, but 1.0 is the magic number.
Even if there's one good vaccine, having multiple good vaccine types in the world will be better. The virus is less likely to evolve a defence against multiple vaccines than against a single type deployed everywhere.
The fact this vaccine targets the spike protein is also good news, because even if the virus evolves, there's evidence that the spike protein is key to its harmfulness, so any evolved strains that keep it will likely trigger an immune response, and evolved strains that change the spike protein seem likely to be less harmful too.
The virus cannot replicate, the genetic material inside the virus cannot create new viruses as in there are no instructions inside the payload to replicate and assemble new virions.
To make the virus for the vaccine you need to use a different virus that when it replicates it creates copies of the actual virus used in the vaccine.
Think about it as a self extracting archive that creates copies of an uncompressed file (the actual vaccine) the file that it outputs doesn't have the information to reconstruct the self extracting archive itself.
I guess the thought is that a really unlucky evolutionary accident would be when the other virus capable of replicating and the vaccine meet in a body, and by chance transfer some of those instructions across. I presume that's rare or never seen, but I don't know, and (with a safety-engineering mindset on) I'd automatically consider that a "chance" unless it is ruled out by something.
Anything can happen however we've been using weakened, inactivated and closely related viruses in vaccines for a long time now without any such natural selection accidents occurring.
From Wikipedia under "attenuated vaccine" (which I know this is not):
> In extremely rare cases, natural mutations can cause a reversion to virulence. In this case, the virus can revert to wild type or develop into an entirely new strain.
Now, the Oxford vaccine is not an attenuated virus as is usually meant by that term.
On the other hand, it's not the same as an "inactivated virus" vaccine type either, where a virus is broken apart.
It's a different sort which doesn't fall into either of those categories. It's described as a "weaken adenovirus" and "replication-deficient" because of replication genes being deleted, and spike protein coding added. (There's no coronavirus at all, just the spike protein. This is completely different from other vaccines.)
The replication-deficient adenovirus has been studied thoroughly, not just for Covid but earlier as well. There are good reasons they selected it.
I will certainly take that vaccine when it's available, if that counts as any sort of endorsement.
I have high confidence in the people engineering and studying it. (I'm in Oxford, btw ;-) But can you really generalise the observations of inactivated virus vaccines to this relatively new kind? I think no, it has to be studied and monitored with care. Thankfully, I think they are doing exactly that.
if we're back to normalish by spring next year I think that would be a great outcome, if the messaging to the public would be, buckle down until then I think lockdown complaince could go up
I think you're vastly overestimating our capacity to build enough vaccines and distribute them over the world, as well as dealing with those who will refuse to vaccinate.
Even if we had a vaccine ready for the roll-out today, I don't see us going back to normalish until late 2021 at earliest.
As with any vaccine, you'd need about 80% of the population to vaccinate in order for herd immunity to kick in. I feel like we're gonna have trouble reaching that amount for years to come.
Getting a working vaccine is only step 1 towards eradication path, not the end goal.
Pfizer is already mass producing their vaccine and are saying they’ll have 100 million doses available this year and are targeting 1.3 billion next year.
The US has five million people who tested positive and have recovered. Likely also another 30-50 million who were never tested because their symptoms were to minor. And another 66-165 million who have cross reactive T-cells.
Some researchers have concluded that the herd immunity threshold for sars-cov-2 could be as low as 10% or as high as 50%. I don’t think anyone sees it as high as 80%.
The mayo clinic suggests it could be 70%, and I have seen others suggest 80%. I have not seen anyone suggest as low as 10/20% so I think that suggestion is a huge outlier and even the paper you link says as much.
There actually has been several papers posted to r/COVID19 that have suggested that the herd immunity threshold is likely overestimated. This is because vulnerability to infection isn't uniform across the population. Some people will be more likely to be infected, either due to biological reasons, like a weaker immune system, or sociological ones, like living or working in an area where transmission is far more likely. Most of the higher estimates of a herd immunity threshold of 70-80% are based on transmission dynamics from early in the pandemic, which mostly consisted of these people with higher probabilities of infection. Once this population starts to get burned out, the transmission of the virus also slows, which means that the herd immunity barrier also drops.
One of the papers hypothesized that this demonstrates why areas like NYC got hit so hard initially and have remained stable since. Seroprevalence surveys back in the early summer indicated that between 20-30% of NYC residents had contracted Covid already. The lockdowns obviously blunted the surge, but unlike other areas of the country, as NYC has opened back up, there hasn't been much of a second wave at all. With more than 2/3rds of the population still without any kind of exposure to the virus, you would expect a dense city like NYC to see a large increase. The paper concluded that this is evidence that might suggest that the herd immunity barrier is far lower than initially estimated. I've seen some papers suggest something closer to 20-50%, but nothing so low as 10%. I'll see if I can dig up some of the preprints to post here.
That's because 70/80% estimates assume that the population is entirely vulnerable, while instead it looks like it's partially vulnerable. Hence the estimates would need adjustment.
80% or so is accurate if there was no cross-reactivity and if asymptomatic is included in the case count. It's what was being reported in March or so when we didn't yet have evidence of cross-reactivity.
In most models, we currently assume herd immunity is 50%. We know it isn’t higher than that but we also have circumstantial evidence that it likely isn’t below 40%. A complicating factor is that we know the number of infections is much higher than the number of cases but we don’t know by how much and this is not something we can effectively measure retroactively, which makes it challenging to model precisely.
Which countries have eliminated the latter 4? I would consider an illness "eradicated" if the vaccine is no longer regularly given. At least 10 years ago (when I was in the field), MMR and Chickenpox vaccines were still regularly administered in the US.
> I would consider an illness "eradicated" if the vaccine is no longer regularly given
Fair enough. I would consider a virus eradicated when the general population gives zero thought to it, and effectively no one dies from it. Doesn't meet the strict medical definition, but I thought the description of "If we get to a point where there's a stable number of daily deaths then we're good" was overly pessimistic.
>I would consider an illness "eradicated" if the vaccine is no longer regularly given.
That's not how it works. Just because you don't see an outbreak for a while, that is never a reason to stop immunizing children. Pathogens can and do have natural reservoirs. This is why when some idiots stopped taking the Measles vaccines we had an outbreak here in the US.
Of course that's how it works. We don't regularly administer small pox vaccines anymore because it has been eradicated except for a couple of very tightly controlled samples. That's what "eradication" means. My memory is slightly hazy, but I think we might have skipped Polio as well for anyone not going oversees, because Polio largely meets the definition of "eradicated" in the US. Meanwhile, we continue to administer MMR and Chickenpox vaccines because those diseases still exist in the wild. The very fact that Measles has returned is ipso facto proof that it was never eradicated, and the fact that (normal) people never stopped giving that vaccine to their kids is proof that no one ever believed it was.
Covid-19 isn't a "common type of flu" either. The diseases I mentioned were certainly widespread and endemic. And they're all different types of virus.
A friend of mine in public health mentioned to me that it's not uncommon for second waves of epidemics to be less deadly, since many of the people most vulnerable to the disease would have already passed away during the first wave.
This idea that the "Media" is this sinister entity trying to stop the spread of good news during a pandemic which the entire world has taken drastic steps to curtail yet which has still killed over 1.1 million people is just so silly.
The media optimizes for eyeballs and attention, and hence we see hysterical, inaccurate, and fear-based reporting. With all the noise they put it, it absolutely does crowds out facts showing that the virus is now likely less deadly than it was in the earlier phase of the pandemic.
It doesn’t “mean nothing”, it’s another data point. If you see test positivity rate remaining low but cases increasing - which we do in many areas with sufficient testing - then it does suggest more people are getting the virus.
You can also corroborate this by comparing it to new hospitalizations, which are also up.
“Deaths is the only relevant measure” - not sure where to start with this except to say that this is not at all what epidemiologists seem to think and I won’t address it further without some very dramatic reasoning and evidence.
” If you see test positivity rate remaining low but cases increasing - which we do in many areas with sufficient testing - then it does suggest more people are getting the virus.”
No, it suggests that you’re doing more testing, and finding more cases. Which, exactly as the OP said, is a metric that can be manipulated by doing more testing.
The whole reason we emphasize positivity rate is to try to compensate for the inherent bias in reporting raw case counts.
There have been far more cases than we have ever formally detected with testing. There’s plenty of room to increase that number by testing more people, but it will not affect hospitalizations or deaths -
which is exactly what we’re seeing.
Deaths are not an entirely useful measure to see how the pandemic is progressing because they are a lagging indicator.
Positive test rates measure what was happening about a week ago. Hospital admissions reflect activity a week or two before that, and deaths often get reported a month or more after the events that caused people to get infected.
You have to look at all the data to get an idea of what is happening.
There has been a slight uptick in weekly deaths, roughly on par with what was observed in the last week of September. Given the trend of the line and the delayed reporting from most states, it’s more accurate to say that deaths have flattened:
Doing so would ignore the sometimes dramatic effects survivors experience - from the people I know alone, this ranges anywhere from previous marathon runners still huffing and puffing their way up stairs despite having been otherwise symptom free for 6 months, to a man who survived by the skin of his teeth and it now appears will never be able to taste or smell again.
I don't know about you but I'm feeling like simply "getting to a stable number of daily deaths" doesn't cut it. Also, that statement alone doesn't make sense to me - a fatality rate of 50% could potentially maintain a stable rate of daily deaths... Of thousands.
Given the low fatality rate for COVID, wouldn't you just want to concentrate vaccination on those most at risk? i.e. the elderly, people with underlying conditions etc.
You don't need to eradicate the virus, just stop it affecting the most vulnerable. Everybody else can then carry on as normal (albeit with a slight chance of getting a nasty flu-like illness).
SARS-CoV-2 relies on superspreading much more than e.g. the common cold. When you hear, for example, that each patient in a given area infects 1.2 other people on average, this doesn't mean that everyone spreads it to one or two people. It means that out of 10 infectious patients, 9 patients don't spread it to anyone else and the tenth patient spreads it to a dozen people at once.
Because of this high dispersion rate, it may make sense to earmark a certain amount of vaccine doses for people who are not themselves at risk of complications when contracting Covid, but who are at risk of becoming a superspreader.
"Just do the vulnerable people first" has the significant advantage of being easy to explain and implement, but it does not maximize the speed of economic recovery.
For instance, I'm a vulnerable person because of preexisting conditions, so I'll likely be offered a vaccine relatively soon after approval. But that won't have a large impact on economic recovery: I'm in the home office in a single-person household and don't have any care obligations, so I'm at a comparatively low risk anyway. And I won't change my current behavior until the disease is fully gone anyway.
My thoughts in treating the vulnerable first wasn't because I thought the vulnerable would then be able to go back out to work, but because the vulnerable would be relatively safe the people with no pre-exisiting conditions wouldn't have to stay home to stop the spread.
Even if we vaccinate every vulnerable group, no vaccine has 100% success rate. That's why every vaccine we ever had relied on a huge majority of people having it to prevent the virus from reaching those whose vaccine failed.
Not to mention that we already know about long term side effects that have nothing to do with a specific age group, and that there's a chance of re-infection.
Sure but it would reduce the number of deaths by a lot.
If we just vaccinated 65+ year olds, we'd cut deaths by 80X%, where X is the effectivelness of the vaccine. Even if the vaccine was only 80% effective, that's still 65% reduction.
Add in people with dangerous conditions, heart conditions, cancer, morbidly obese, etc., and you could probably knock it down further.
And as the percent of the population with immunity rises, the spread will slow quite a bit.
As with any vaccine, you'd need about 80% of the population to vaccinate in order for herd immunity to kick in.
Wrong. The herd immunity threshold (HIT) for influenza is 33%-44%. HITs are different for every infectious disease. Current estimates for COVID-19 are 60-75%.
Isn't that a different number, though? You have to factor in that vaccines aren't 100% effective at preventing disease. Wikipedia spells it out in the vaccine section here [1]
True but you're also not taking in to account that far less than 100% of the population appear susceptible to the virus, especially in e.g. Japan and Germany, for various reasons.
Do you have a credible source? I've heard these claims multiple times and they done seem to be borne out by events or supported by repudiable epidemiologist.
Furthermore, I know of at least 3 leading statisticians that hypothesized (very early on) that the variance of infection trends pointed to pre-existing immunity in various populations. The evidence supporting this is mounting.
The BMJ is not a credible source, it is the Daily Mail of medical journals. The author of that article, Peter Doshi, has form:
"I think the first thing we to review is who is Peter Doshi? And why is he so insistent on getting this data?
Peter Doshi received his BA in anthropology from Brown University, MA in East Asian studies from Harvard University, and Ph.D. in history, anthropology, and science, technology and society from the Massachusetts Institute of Technology. Those would be fine credentials for someone who is going to teach history or anthropology."
I didn't cite the BMJ as the source, but nice try. The sources include Cell and Nature, but unfortunately for you that might mean having to read something in order to discount it, which you seem unprepared for.
That paper looks at 40 people and has no idea what the clinical correlates of the non-spike responses are because no one has any idea. You cannot take that paper and say that a substantial factor of people are protected due to preexisting responses.
COVID is special though in that if it were only as deadly to the young as it were to everyone, I don't think we'd be referring to this as a pandemic.
Literally, right now we are seeing case rates explode, but the number of casualties is paradoxically very low because it's mostly the younger cohorts getting sick - which is probably a social function of things like 'back school' and 'risky behaviours' among younger groups.
If we could get everyone 50+ vaccinated, we may be largely safe - maybe not 'back to normal safe' - but the combination of 'partial herd immunity', 'much lower rates of hospitalization' etc. may mean we can 'kind of get back to normal'.
> Some of the longer term effects are scary though - I suspect that younger people might not be so blasé about chronic illness.
There's not a single peer-reviewed study showing a significantly higher frequency of long-term adverse effects in healthy individuals compared to other respiratory illnesses.
There's initial results that indicate that its likely - you wont get hard data for another decade plus - but take it from me you don't want to get CKD or similar organ damage.
But notice, in the latter chart, that in the US the number of infections is predicted to peak in January and then start going down. It seems plausible that by March, we'll achieve some level of herd immunity, relative to the precautions that are currently being taken. We might have a situation like Europe over this pas summer, with small numbers of cases until a second spike in Fall/Winter 2021. That would buy us the spring and summer to roll out a vaccine.
Of course, I'm far from sure that this is what will happen -- but it certainly seems plausible to me.
It's been estimated that 80% of the population needs to have been infected to achieve herd immunity. That means ~240 million people in the United States need to be infected. We're at 8.7 million infected. No way we get herd immunity anytime soon.
For example, I'm a professor at the University of South Carolina. Here we've had around 2,500 confirmed Covid cases, and perhaps around 10,000 cases in actuality. Nearly all of them happened in the first few weeks of the semester, and now the positive test rate is extremely low.
Looking around town, it's pretty clear what happened. There are some students that have acted like nothing is happening, partying and drinking constantly. That population has presumably hit herd immunity already. Meanwhile, there are many students (and staff) that are exercising precautions, and not venturing out a lot, and probably few of them have contracted the disease.
Now, we can't just go back to normal, or else cases would spike among this second group -- but locally it seems that we can afford to relax a bit.
And, also, we're at 8.8 million confirmed infected -- the actual numbers are presumably much higher.
None of the vaccines currently on the table are even remotely good enough for 'back to normalish.' The attack rate for this virus is so high that a vaccine good enough (i.e. multiple 9s effectiveness) to allow 'back to normal' almost certainly isn't possible.
The most we're going to get out of a vaccine is a tool that can be used in conjunction with physical distancing, and masks, to keep the infection rate and hospitalization rate sustainable.
Even with a vaccine, COVID-19 will remain one of the leading causes of death among the sick and elderly. The percentage of chronically ill people who live, and the percentage of people who make it past age 65, will plummet.
Everyone who's alive now will almost certainly need to socially distance (and should wear an N95/KN95 mask in public indoor spaces) for the rest of their lives.
> None of the vaccines currently on the table are even remotely good enough for 'back to normalish.' The attack rate for this virus is so high that a vaccine good enough (i.e. multiple 9s effectiveness) to allow 'back to normal' almost certainly isn't possible.
Is it? Current studies, AFAIK, give very variable attack rates, from low zeros to around 30%. Only higher if due to close contacts for longer periods of time (carriers, fishing boats, meat packing plants). This preprint on trasmission dynamics and evidence from September[1] has lower figures.
> Everyone who's alive now will almost certainly need to socially distance (and should wear an N95/KN95 mask in public indoor spaces) for the rest of their lives.
I wonder how we're even supposed to build a society that can live without any or very reduced form of contact. I think it's socially unsustainable.
No offense, but this is one of the worst comments I've ever read on hackernews. You have not a single piece of evidence for any of your claims, and they fly directly in the face of all reasoning about how a disease like this is most likely to work once it becomes long-term endemic.
A disease isn’t something you can solve by pretending really hard that it doesn’t exist. People getting their news from irresponsible politicians get sick like everyone else, and that’s why it won’t get back to normal before there’s a vaccine or very effective treatment: it’ll be the same cycle of open-spike-close and businesses not having enough customers to be viable.
>A disease isn’t something you can solve by pretending really hard that it doesn’t exist.
This is demonstrably false. Some places are already back to life as normal, like Florida and Sweden, with no business closures. And in spite of this they still have lower deaths per capita than some places with heavy lockdowns like New York, Peru, Belgium and Spain.
Come on. Florida is not "back to normal". The health department is still advocating the full suite of social interventions for citizens, including masks & social distancing.
> it’ll be the same cycle of open-spike-close and businesses not having enough customers to be viable.
That's the part I'm referring to by "not caring" - just ignoring the close orders, especially since "two weeks to slow the spread" has been so completely abandoned.
Ignoring the law doesn’t lead to normal: just more preventable deaths and bankruptcies when businesses burn capital trying to stay open without enough customers to be profitable, even assuming they avoid legal repercussions.
* What law? In the US, the lockdowns were under emergency powers of the executive branch, which are supposed to only last a limited time (30 days where I am, for example). Several of these were challenged and found to be unlawful.
* The US lockdowns were originally only mean to prevent hospitals from being overloaded. We are way way past that point where that was an issue - all the emergency capacity has been dismantled for months.
* As sibling comment implies, something like half the states in the US aren't under any lockdown now, businesses there aren't having issues staying open, and their stats are no worse than the locked-down states.
* Speaking of preventable deaths, suicide and overdose are climbing where lockdowns are still in place.
In the U.S., the lockdowns were issued in compliance with local laws. As you could easily learn for yourself, those vary from state to state and city to city so you can't make a blanket statement without being incorrect. In the context of this thread, you specifically referred to “ignoring close orders” which implicitly acknowledges the existence of an order issued by someone with the authority to do so under current law.
In some cases there have been legal challenges to those laws so there aren't givens but even if those are successful, my point was that even if you do re-open you can't force customers to come back when they feel unsafe. Even in the states where restrictions have been relaxed, a large number of people are not comfortable hanging out at a bar or restaurant — the problem being the risk of a serious disease, not the countermeasures deployed against it.
> The US lockdowns were originally only mean to prevent hospitals from being overloaded. We are way way past that point where that was an issue - all the emergency capacity has been dismantled for months.
The lockdowns were, as clearly communicated at the time, intended to slow community spread. Avoiding hospital overload was part of that but so was avoiding large numbers of people getting a serious disease with potentially life-changing impact when they don't need to.
> As sibling comment implies, something like half the states in the US aren't under any lockdown now, businesses there aren't having issues staying open, and their stats are no worse than the locked-down states.
And that commenter was wrong just like you are wrong. Anyone who follows this issue knows that the cases have been rising recently (~35%) and there's a noticeable correlation with the states which re-opened high risk activities and those who did not.
For example, they mentioned South Dakota which is at an all-time peak:
A common cause of error here are people looking at the all-time cumulative stats rather than the last week or two and missing that while, say, NYC was hit early with quick community spread in a dense environment and thus had a brutal spring but the increased lockdown have kept levels low since then.
Unfortunately, that’s not how a disease with a likely limited duration of immunity works. Also, the knock on effects of uncontrolled spread over the winter will almost guarantee that next year won’t be normal across many domains.
It likely won't be available to everyone in the US until Autumn timeframe. Perhaps even later if the vaccine needs repeated dosages over time. Priority will be health care workers, essential retail, vulnerable etc.
By then it will kill at least a million people at the current trajectory. So US needs to start acting more aggressively now.
> Two of those companies, Moderna and Pfizer, are now in Phase 3, large-scale clinical trials. The 30,000 volunteers in each of the trials are getting two doses, with Moderna spacing their shots out 28 days apart and Pfizer spacing theirs out by 21 days.
> AstraZeneca is expected to start Phase 3 trials this month. Their Phase 1 and Phase 2 trials used two doses given 28 days apart.
A: Quite data driven (and frustrated when data's not there)
B: Former work history in monetary policy a fan of fan-charts (i.e. central projection isn't the only thing, there is a spread from the central projection).
C: Not willing to over-speculate on either side.
D: Perhaps not a super people person, but not negative either, see A. Quite nuanced if others listen, and would listen to those advising him keenly. And starkly aware of causes of death that are not Covid-19, but linked and accelerated due to it - avoiding hospitals, mental distress, etc.
All in all, not a bad choice for a health secretary. Reading between the lines, I'd give it 2-3 months until this is rolled out.
>OK, someone tell me why this isn't the good news it sounds like
The AstraZeneca vaccine is based on an adenovirus vector, which has never been approved for use in humans. It uses a weakened live virus that can (and apparently has, in the case of the J&J vaccine, which is using very similar tech) cause serious adverse systemic reactions. From what we've seen so far, the safety profile for these vaccines is far worse than the mRNA/lipid nanoparticle based vaccines coming from Moderna and Pfizer/Biontech.
It's also not really news. We know that a vaccine will prompt an immune response. Dozens of others in progress have already shown this with phase 1 and phase 2 data. The question is how strong, how long lasting, and how safe is it, along with the question of real world efficacy data from placebo controlled trials.
> It uses a weakened live virus that can (and apparently has, in the case of the J&J vaccine, which is using very similar tech) cause serious adverse systemic reactions.
There is no evidence to prove the vaccine has caused any serious adverse effects so far. If that were the case, it is unlikely the Data Safety and Monitoring Board (DSMB) and U.S. Food and Drug Administration (FDA) would recommend resuming the trial.
> After a thorough evaluation of a serious medical event experienced by one study participant, no clear cause has been identified. There are many possible factors that could have caused the event. Based on the information gathered to date and the input of independent experts, the Company has found no evidence that the vaccine candidate caused the event.
>There is no evidence to prove the vaccine has caused any serious adverse effects so far. If that were the case, it is unlikely the Data Safety and Monitoring Board (DSMB) and U.S. Food and Drug Administration (FDA) would recommend resuming the trial.
There's also no evidence to prove that it wasn't. Furthermore, the AstraZeneca vaccine was halted for a case of transverse myelitis, a very common (and serious) adverse reaction seen in DNA/adenovirus based vaccines like ChAdOx1 [0]. These complications have not been seen at all in the mRNA based vaccines, since they do not involve a live virus.
The worrying trend is the ,,signed contracts with governments'' part even though the clinical trial results are not out yet. It seems that vaccination gets highly political, just like how EU made a mistake of paying for Remdesivir even though we knew that it's not worth it at that point.
It's great news, though at first I thought they had released Phase 3 results, which would be earth-shattering news. They are still the leading vaccine candidate and the one most likely to get approval this year (though the US press tends to ignore it in favor of covering the various US-originated vaccines that are also in Phase 3 trials).
I care about what I can personally get for my family. We are low on the list (able to stay home almost entirely unlike health care or retail). We are tired of this, and no end is in site. The US origin vaccines (some of them are one shot or require less care in handling seem like the ones that we need)
It is good news, but it's not earth shattering. This vaccine produced an immune response (the the vaccine antigen), which many of the other candidates have as well. The real question is, will it prevent infection? Those are two different questions.
Glass half full: We can measure an immune response also in populations where it's more difficult to get a decent one. An immune response means that the immune system actually is taking action against the viral antigen.
Glass half empty: We don't know how the immune response measured relates to protection from or lessening of the infection. This is what the ongoing trial is trying to find out.
This is, IIRC, the second report of successful immunogenicity in older people. There was a (small) cohort of > 65 year old people tested with Pfizer / BioNTech's vaccine in the Phase 1 trial, and even there immune responses were found and measured.
There are tests that can be run to show an immune response.
One thing I’ve learned is it’s extremely hard to get doctors to run the tests.
AND there are a whole lot of them.
AND
I’ve run into many doctors that are 10-20 years out of date with treatment and diagnosis protocols.
As in, current recommendations are that test X isn’t reliable. Use test Y.
Doctor refuses to run any test because you’re the wrong gender.
AND
The moment you see someone in a practice your banned from seeing anyone else in the practice. So second opinion means going to 20 miles to another center.
Oh, and it’s 3 months+ to get a single appointment. You may need two dozen appointments until they narrow in on the issue.
That something is possible still leaves a massive gap of getting it done.
Likely long-term results are not known yet. We've already had one vaccine potentially causing side effects that stopped the human trials for a while. (I think it was the Russian one. Please correct me if not)
It was the UK trials of the Oxford and AstraZeneca vaccine after 1 person experienced an adverse reaction - but that's the whole point of the trials and not uncommon so no major worry there, and they were restarted soon after.
It’s just a political thing. You see the same behavior in threads about climate change. A seemingly innocuous comment to you is a firebrand political statement to someone who thinks the virus is a hoax or whatever.
AstraZeneca has agreements with all governments whereby they don't claim any responsibility for the vaccine. It's the national governments that will deal with any side effects.
It's fair if the degree of disclaiming is proportionate to the need and the pace.
They shouldn't be off the hook completely. They should still have to show they have conducted a responsible level of testing and checking for the circumstances, that they are continuing to refine that verification even after widespread deployment, and to motivate that to be done all levels requires some degree of moral hazard remains in place for them. In other words there should be some sharing of risk. Imho.
They are still going through clinical trials its just that getting to that stage has been accelerated.
So this isn't like we are relying on AZ to create it, test it and sign it off. National agencies will ultimately sign off on whether it can be used or not. Given the high profile nature of this vaccine you can be sure that results will be widely studied, and the opportunity to hide results they don't like will be limited given we all know the trials are occurring.
I think they're mostly producing this on a break even/no profit basis for at least the initial roll out?
If there is some sharing of risk, but no profit to be had (and ultimately profit is what buffers you against risk) then why would you be involved at all? Let some other company take the risk?
That's the responsibility of the FDA, EMA etc., to make sure all of the above is met. However to be open to vaccine injury claims, in the current societal climate (lots of malicious actos and antivaccine disinformation among the public), would risk the financial viability of vaccine makers. That's a longtime problem in the US (hence some of the vaccine makers are protected by the National Childhood Vaccine Injury Act) and other countries.
Now (soon, hopefully) people can acquire immunity through a vaccine, instead of through a virus that leaves long-lasting damage to the body (in particular, but not limited to, the brain).
> leaves long-lasting damage to the body (in particular, but not limited to, the brain).
In what percentage of people who get COVID-19 is there long-lasting damage to the body? What other conditions did the people who get long-lasting damage to the body have? How does these numbers compare with other diseases?
Most people with COVID even with few symptoms have a loss of smell. If you like numbers, I read that around 80% of people with COVID report loss of smell.
And this is one kind of neurological effect. This is a more global view of how the virus could affect the brain:
> One in 20 people with coronavirus are likely to have symptoms for eight weeks or more, according to a new study by King's College London.
> The research, which uses data from the COVID Symptom Study App, suggested so-called "long COVID" affects around 10% of 18 to 49-year-olds who become unwell with coronavirus.
From your first link: 10% had any symptoms lasting longer than four weeks. That’s not “severe long-term effects”.
The actual study seems to say 1 in 20 have symptoms for eight weeks, which might be closer to what you could fairly describe as “long-term”, but says nothing about the severity (though I haven’t waded through the whole article).
Anyway, the drop-off from 10% having symptoms at 4 weeks to 5% at 8 weeks is encouraging - it intuitively suggests that the negative symptoms aren’t permanent, even if they take a long time to go away.
Yeah, last time I was sick I had the flu. I had lingering effects for around 8-10 weeks after. Eventually I had to go to hospital to get checked.
I feel a lot of Covid effects are being massively overblown because people aren't aware that other more common viruses that we don't worry about can have these "long term" effects as well.
People aren't worried about 8-10 weeks of lingering effects.
Those 4 week and 8 week statistics are part of an attempt to understand what's going on. It doesn't mean 8 weeks is considered long covid.
They are worried about effects where people got it months ago and are still disabled from it. Things like still struggling to walk upstairs 6 months after getting covid.
And that young, fit people are reporting it, not just "old".
The worry is that it doesn't appear to be getting better for them yet. The greatest worry is that people who get it might never recover, or might take years to recover. We can't know yet.
Flu and other viruses affect some people that way, but it's a small number of unlucky people. The worry is that the number affected by long covid in this way are a much larger number of people.
I have a colleague who is essentially disabled from it & has not returned to work, after 8 months, so I have first hand experience of what you speak.
My fear is that this is super, super, super rare, but figures are including long term as low as 8 weeks, so we have absolutely no idea how small / large the number of people having this critical level of long term effect actually is.
> Most people would worry about 'long term health effects' as they'd usually assume that it's going to go on for years.
There are plenty of anecdotes to be found of people reporting debilitating long-covid symptoms for 6 months so far. That's "still sick since I had it back in March/April".
(It hasn't been around for a year so nothing can be said about that timescale yet.)
That's significant enough that public health officials are talking openly about it as a concern, so it's not just a few isolated anecdata.
There are some reports suggesting neurological impairment. Along with observed blood changes (thickening), which is concerning regarding long term damage for rational reasons. If that turns out to be true, that sort of damage tends to never completely recover. Rather you learn to adapt and live with it.
Yes, my colleague is one of them. He has still not recovered after 8 months and is unable to work.
However, they stating they're also counting 8-10 weeks as long term, so the stats are obviously way inflated. I'd really like to know the number of people having the extreme effects, without the media trying to inflate the figure.
As well as acquiring immunity without being infectious.
However, the efficacy of this vaccine (and all the other candidates) still needs to be clarified - ie is it like a measles vaccination (~90% efficacy) or the flu vaccines (~ 25% - 50% I believe).
For the FDA to even consider an emergency use authorization, they have put the following requirements:
- Efficacy of at least 60%
- Lower bound of efficacy (confidence interval) >= 30%
- Minimum safety data for at least one or two months post vaccination (I don't remember if it's one or two)
- At least five severe cases in the control arm
- Requirements for the trials to go on even if efficacy is found for an additional year after the trial end (for most of the trials, this means two years in total)
Judging from our response to Covid-19, if this had actually been the collectively-feared zombie virus, the pandemic would have been far worse than any fictional account has manage to capture so far.
Future zombie apocalypse stories need to include people who deny it as a hoax, blame it on foreign countries, claim it's just a mild flu, just continue partying as if there's no risk at all, claim it's caused by 5G technology, claim it's a conspiracy by the elite to accomplish whatever, and political parties split on the topic.
Also if there was a real zombie virus none of the movies so far have captured the sheer absolute terror of hard to defend transmission vectors like mosquitos, which would be likely to get the virus. Brings a whole new level of issues to not getting bit.
As science fiction is speculative, I do not fault any of those listed media however I feel none of them truly captured the sociopolitical insanity that would occur, the sheer level of ignorance and incompetence which causes anything that could go wrong, to go wrong.
It's a surrogate outcome.
"Prompts immune response" means "we hope it prevents infections". It doesn't necessarily mean it will.
This is still good news. But it should be put in perspective, this does not automatically translate to "this vaccine will work fine in both young and old". It just means we can have some higher hopes that it will.
Only RCT results of the real infections will show if it really works. (RCT for the vaccine is running and first results are expected soon.)
Randomised Controlled Trial - essentially, take a population, give half of them the vaccine, and half a placebo, and study the reaction.
What you're referring to (voluntarily infecting people) are challenge trials, which are also being discussed, but are still somewhat ethically dubious.
Wikipedia tells me RCT is "randomized controlled trial", that thing they are doing where half the volunteers receive the experimental vaccine and half receive a placebo, and they wait to see how many get the disease (and how many get side effects) in each group. I don't think there's any "human challenge study" (in which they deliberately infect the volunteer, https://en.wikipedia.org/wiki/Human_challenge_study) so far.
RCT = randomised controlled trial - a trial where some test subjects are given the vaccine and some are given the vaccine, then you follow the subjects and see which ones get COVID and how bad.
There are already a bunch of vaccines going through this process.
Challenge trials is where you purposefully infect subjects. TheY are highlY controversial but according to Oxford, would speed up the research and they are planning to do one.
Because by the time this passes clinical trials the Chinese vaccine will have been in mass production for months. The FDA will delay adoption of any vaccine in the US for many months in order to keep to the same standards they use when the world isn’t on fire.
The bad news is that we can't really have one vaccine candidate released to the general public much before the others, as that will impact the results of other vaccines that are still in Phase 1/2/3.
It is good news if true, but we are rushing the trials of a new vaccine and then potentially going to give it to a large number of people. What if the vaccine has long term negative effects?
While long-term side effects are theoretically possible with any treatment, this vaccine is based on a platform that's been safety-tested repeatedly in experiment vaccines for prostate cancer, MERS, malaria, tuberculosis, influenza and chikungunya virus, so there's a lot of past safety data. In addition because the main effect of the vaccine is to trigger a strong immune response, you would typically see side effects in the short term related to that initial response (things like Guillain-Barré syndrome or Transverse myelitis), not over the long term as the effect wanes.
Because a vaccine that provokes an immune response isn't the hard part. It's making sure it doesn't make people sick, and then scaling it to producing and distributing hundreds of millions of doses.
I mean, its better news than the alternative, but I think "Oxford vaccine produces zero immune response" would be a far less likely outcome.
It is the same. But you cannot expect a vaccine to work similarly in people of two different regions having major differences in their diet, climate and lifestyles. That's why many vaccine candidates are being tested in multiple countries( read potential markets).
Also, I think the UK has preferential rights at least on the initial yield of the vaccine.
> But you cannot expect a vaccine to work similarly in people of two different regions having major differences in their diet, climate and lifestyles.
Can you? Do you have any examples of successful vaccines that are only given in one region because they have been proven ineffective in a different region?
Not knowing anything about big pharma, does Astrazeneca make all the money here? How much does a vaccine like this cost per person given the scale of the distribution and manufacturing?
Usually there is an IP agreement. Also, ever notice the media calls it “Oxford study/vaccine” for good news and “Astrazeneca study/vaccine” when it’s bad news (like a few weeks ago when they had to shutdown to multiple people getting an unknown illness).
I work in an area where we make agreements with university’s. It’s often shared IP or publicity. Alternatively, one can publish, once the other makes profits. Or it could be something in between.
In this case, I bet everyone is doing this pro-Bono from a future profit perspective, because the government is paying for all of it.
IIRC, the expected price is around $3.50/dose, but I can't find the source for that anymore. AZ and Oxford have pledged not to ask for royalties or whatever, at least until the pandemic is ongoing (that would likely mean all of 2021 at the earliest).
Good news but still a long way to go. How's it going to be rolled out? Here in the UK we have tried and failed to get a regular flu jab (our GPs have run out of a very small supply and the pharmacies don't have any to sell) and I'm not optimistic about our chances of getting this next year or whenever it arrives.
I think you might be surprised. The government knows that this is the silver bullet they need to rescue the economy from oblivion.
I’m expecting that once this thing is ready there’ll be a logistical effort for the history books to roll it out. See what they can do with the military involved, like the nightingales.
Sad to say, given how testing, lockdown, etc. has proceeded, I'm losing confidence that most western governments are capable of any "logistical efforts for the history books" at this point.
I heard a lot of bluster about testing here in Ontario in the spring, but here we are in the fall with rationing of tests again.
I suspect the government will magically be much better at logistical efforts when there's a clear economic pay-off. Neoliberalism might not be great when it comes to helping the little man, but I suspect it can swiftly get its act together when it comes to a short-term solution to economic malaise.
For what it's worth, our testing has steadily increased since then. Perhaps we ought to expect more than "steadily", but the recent rationing is more to do with dramatic uptick in demand for tests (schools reopening, immediately followed by Thanksgiving) than with a change in capacity.
Testing in Waterloo Region was really good over the summer— minimal wait times, multiple drive-in sites, results turned around in 24-36hrs. I think they just failed to account for the bump that would come from school starting and people wanting to get tested in advance of Thanksgiving.
I think the "military involved" piece is key, especially if you're talking about the US. It's maybe a bit trite at this point, but a lot of comparisons were made about the stark contrast in how quickly a national response mobilized in response to BLM protests vs the pandemic. The basic takeaway being: executive priorities matter, and even Trump has made it clear on a number of occasions that getting the vaccine out is important to him.
I guess that's the thing; the gov't is the one who made the decision to bring kids back fulltime, how incompetent do you have to be to not know there'd be a bump in testing demands?
Re: Waterloo region, I work at Google Waterloo, so although I don't live in KW (I'm in rural Flamborough) most of my coworkers do. I had one who showed up at 7am to get a test, lineups were around several blocks and they shut the whole thing down because people were getting rude. He then had to wait a bit and drive to Guelph. People were driving out from Toronto to London, Woodstock, etc. to get tests.
In our industry if we provisioned data centres or server instances like this, we'd be in a bit of trouble, no?
EDIT: FWIW I have a political leaning and bias towards a strong public sector and am a big believer in public service. I'm not one of those "government can't do anything right" and "less government is better" types. But I do think that several decades of "government can't do anything right" people being a dominant cultural and political force now means that government can no longer do anything right. We're losing our ability to act collectively :-(
I like Horwath but I think her admin would have faced insurmountable ideological opposition, the same way Rae did. And then the whole COVID response would have been framed in those terms, as a right-left politicization like it is in the US. At least now, with a right wing government administrating the COVID response, only the far lunatic right (cough Randy Hillier cough) has politicized it. For conservatives, it's "their guy" delivering the tough medicine, and they just blame Trudeau for anything they don't like, even things the feds have nothing to do with. While it hasn't been great the management of this situation is not _nearly_ as bad as it could be. Just look at Jason Kenney's gov't.
Can I check: are you in the priority group for flu jabs?
Because GPs (in England, I don't know about the other nations) should have enough stock. They are prioritising higher need first, and then the expanded programme later in the year, and then anyone else who wants one after that.
If you're not priority need you can try a pharmacist.
According to my GP they had a batch for the over 65s but they ran out pretty quickly. I usually get free flu jabs due to asthma but although it's strongly recommended I'm not aware of it being a definite priority group.
Suggest trying again with your GP. I'm also in a lower-priority group and didn't get the jab during the first round, but my local surgery contacted me later when stocks had been replenished.
Aside: It was, for the NHS, an exceptionally efficient process. I was given an exact time slot and was in and out in less than three minutes.
It's actually an "indeterminate way to go". Assuming it is "long" has no factual basis. Phase 3 results could be released literally any day now, and good results would lead to government approvals in the following weeks.
I'm not sure if I can share details but there is emergency vaccine work going on in the UK. The NHS has been using the winter flu vaccines this year as a way to test systems for future rollouts, such as a covid vaccine.
They are manufacturing it already supposedly. But I think the current UK plan is not to vaccinate everyone, but to start with the high risk groups. Perhaps they will then expand out to everyone else later.
They have massively expanded the flu jab programme in the UK this year (to try and avoid hospital overloading) so thats one of the reasons flu jab is in short supply. Apparently its mainly a logistics problem, the doses are there, somewhere, see: https://www.theguardian.com/society/2020/oct/04/gp-surgeries...
Here in Canada we were able to get our flu shot at our family doctor's last week, but it was kind of a "first come first served" and "you have to ask about it" scenario. My employer usually does a flu shot clinic at work every year, but as we're all home we were not able to do that. In some ways there's been more barriers to getting it than in previous years, despite it being more urgent to do so.
If this was rolled out properly people would be actively contacted by phone, etc. with assistance on how to get it. That's the kind of aggressive roll-out I'm hoping we see if/when a COVID19 vaccine becomes available.
What sources are you using here? The UK has one of the best vaccination coverage rates in the world, and the largest ever roll out of the winter flu jab is well underway (reaching a record breaking ~50% of the population).
One interesting point that I read about the Oxford vaccine is that it only needs chilling to -5c. Whereas many of the other vaccines (I don't know if all others or just some) need chilling to -60c. It strikes me that the Oxford vaccine has a distinct advantage when it comes to global distribution.
I'm concerned that, given both effectiveness & willingness to get a vaccine, we may only experience incremental improvements in transmission rates.
The flu vaccine is generally about 50% effective, and only about 50% of (Americans) say they will definitely or probably get a vaccine. If that holds, then combined, that would only cover 25% of the population. Well below herd immunity.
Yes, it would be an improvement, but we should really be embarking on a heavy public awareness campaign that, once available (and assuming a low risk profile) that vaccination is the responsible and safe thing to do.
Basically, there are reasonable estimates that the range could be anywhere from 20% - 70%.
The effect also greatly depends on which portion of the population gets vaccinated. If (in an imaginary world) the most at-risk 50% of the population got vaccinated, we could reasonably expect Covid to actually become something like the flu.
Finally, I expect this is something that'll gain acceptance over time. There are some not unreasonable factors that could cause people to be nervous about a Covid vaccine initially, that will be softened over time. Things like it being developed under the supervision of politicians who could be motivated to rush it out, or just being developed faster than any vaccine ever.
Or, on the flipside, continued travel restrictions for individuals who haven't been vaccinated. Americans traveling to certain tropical countries have been required to get specific vaccines for years, I wouldn't be surprised if over the next few, travel to Europe or even Canada requires a Covid vaccine.
One vaccine doesn't even trigger the same immune response in different people, so it is not entirely clear to me what you mean.
The basic principle of a vaccine is that it contains proteins that are the same as (or similar to) some of the protein building blocks of the actual virus. Your body learns an immune response to these proteins, which it can reactivate when it encounters the real thing.
Many potential vaccines target the same spike proteins on the outside of the virus. I guess you could say those produce "the same immune response" in that sense.
Not the "same", but according to a Nature review on vaccines from last month, most vaccines exhibit a very strong immune response (usually, for the two-dose regimen, after the second shot).
The nature of the response varies. Some candidates are more efficient at eliciting the production of antibodies, while others also activate cellular immunity (T cells).
No. AFAIK, they may target different proteins on the virus hull and also differ in other respects among each other. Some of them might be less effective than others, some might be more prone to being rendered ineffective by virus mutations than others, there can be substantial differences in the number of complications caused by vaccination, and some of them could also cause problems with developing future vaccines for deadly coronavirus variants that may occur another time.
At least, that's how I understand it from what I've heard. Others should please correct me if I'm wrong.
How many people are in the trial, is the fact that two of the responses on this thread are from trial participants indicative of a bias towards nerds in the selection?
I am assuming Pfizer will beat them then? They are expecting approval at the end of November if I recall it correctly and will probably push their stock
I'm a native English speaker (American) and have thought it was odd for a few weeks that Reuters in particular likes to use the word "jab" for "vaccination". It's not commonly used that way in the US.
It's a holdover from print news media to use uncommon-but-short synonyms in headlines. There might be some benefit online as well, but since it's an established jargon/vernacular/dialect/etc of English, they probably just continue to use it out of habit.
It's mine, and the one I study. I'm guessing it's slang for injection? Looking it up now...
I sympathize with your pain of learning a new language (or system or whatever): It's hard to tell if it's a mistake on their part, a mistake on your part, some kind of regionalism, some kind poetry...
The point is that we should reconsider giving (temporary) monopolies to companies that are based public research.
I suggest that we should give merek the for profit monopoly, but allow for non profit manufacturing. If another organization wants to make the vaccine but not derive profit from the process, let them.
Manufacturing takes time and money to develop. Revenue should pay for those costs. The non-profit gains experience, but no profit. The for-profit gains profit. If the for-profit decides to raise prices too high, there will be a willing and capable competitor waiting in the wings.
This is completely incoherent. Consider a book author who has a monopoly on for profit publishing, but anyone else can publish for no profit.
The book author’s expected profits would plummet as it would be the wild west in production.
What you’re really saying is “we should pay massively less for vaccine development”. Which again, sounds nice, but....why would anyone have developed a vaccine? It’s a complex project which costs billions and has taken 12+ months while taking resources away from competing projects.
The public money is an incentive to get people to put those considerations aside and devote all their resources to vaccine development. This is a sensible public investment in a return to normalcy.
Exactly. The idea that the public funds research, but corporations can monopolies the results of that research for profit, is just disgusting. Non-exclusive deals are fine. Exclusive ones not, at least not within the country/countries that funded it; they already paid for it, and denying them access is basically theft.
Drug companies also fund their own research, to the tune of massive expenditures. What you’re suggesting would incentive these companies to disengage from partnerships involving public funding. Whoever pays for the research, each company’s goal is to profitably sell a non-generic treatment. If the only way they can do that is to eschew public funds, they will do this and the result will be less cooperation and a far reduced ability for the government to influence the direction of private sector research, and more importantly shape private sector manufacturing and the quantities of specific treatments supplied to the market.
Honestly, this is overblown. Most of the budget for these corporations goes to marketing, and the R&D mostly goes to repatenting efforts or incremental repurposings. They rarely come out with anything new, and if you look at recent years you may as well say that they never do.
You hit the nail right on the head. This is the same with basically every consumer product in capitalism, which is why it’s so inappropriate for life saving medicine.
The article that graph comes from indicates that is self-reported data from the companies which may not be consistent in what is considered R&D vs. marketing cost.
Maybe I'm mistaken here, but one such case was Sofosbuvir and its pricing was indeed very controversial.
Rant. Prime time TV is now pharma pushing their drugs with the occasional programming jammed between the ads. All those ads are coming from their extreme markups. Placebo and manufacturing artifacts aside, a molecule is a molecule, buying generics should be the default.
It is bad enough, but the real disgrace is pharma salespeople masquerading as GPs prescribing meds according to who is sponsoring them. Instead of telling people about the active ingredient they send them to buy BRAND. At least this is my experience in the 2nd world.
> I suggest that we should give merek the for profit monopoly, but allow for non profit manufacturing. If another organization wants to make the vaccine but not derive profit from the process, let them.
Not-for-profit manufacturing would have to be done by the government itself, wouldn't it? Otherwise, what other entity would and could actually pay to set that up?
Non-profit companies exist all over the US. Even non-profit drug manufacturing is done to some extent, but at a much smaller scale right now than we could have. The companies still charge money for services, the employees get paid, but the governance of the company is not focused solely on increasing profit margins. Most medical core science is done non-profit right now, at US universities. Many universities have on-premise small-scale manufacturing capabilities which serve their own needs, in medical labs but also others, like materials sciences and chemical science/engineering. There's no intrinsic reason why those couldn't be ramped up, or even pooled between physically close universities by creating a joint non-profit entity.
Patents are one tool to promote the progress of science and useful arts. Publicly funded research is a different tool. Usually, patents are based on privately funded research.
the problem is for a competitor to emerge, they have to do a lot of work after X years.
My proposal is to have a company parallel develop processes so we can have competitor after expiry immediately. The competitor can't profit from it, but it can do work at 0 cost.
Society at large is being asked to make drastic adjustments because of a collective health issue.
Why is the corporate "right to make profit" sacrosanct when nothing else is?
This is a clear case of Eminent Domain. All mandated, mandatory, Covid-19 related products must be offered at cost, or even better, we should just nationalize drug companies. We're all in this together and companies need to adjust to "new normal" as well.
This is not corrupt. It’s money well spent. The benefits to us all are most likely more valuable than anything we’ve spent on vaccine research. Government balance sheets also probably come out ahead on that investment given that the alternative is an economy with a raging pandemic and resulting lower tax base.
Then there is the logistical effort of manufacturing the vaccine at the scale and speed required. There are huge capital investments and risks associated with doing that. If a company wants to do that and seek the profits from that, great.
Literally everyone comes out ahead. You, me, the government, the manufacturer, distributor, and every other business or person in the economy.
What is the alternative? We create a government agency that specializes in manufacturing and distributing pharma products?
Not when it's a monopoly. That means the company gets to exploit the results of the research for their own profit, without any competition to keep prices reasonable. Non-exclusive deals are fine. Exclusive ones are not.
Look, I understand the frustration but they're not going to set this price. This thing is way bigger than this company and even the entire pharmaceutical industry. This is a global crisis.
Many governments have proven that they will put the public's need over these companies need. They've broken patents and pressured companies before and they will obviously do it again.
There are more governments in the world than the American one.
For now speed is of the essence and this it's wonderful news they've set another step.
I'm not a public policy, legal, or economics expert, but I certainly favor treating this as a one-off. If a legal monopoly is the most expedient way to get us back to normal, so be it, and if fears of price gouging are a concern let congress or the executive or whomever cap the price. Once things get back to normal we can litigate the monopoly issue.
That’s a fair point. I guess my underlying assumption would be the government funding the research would retain rights to the research as well. Thanks for pointing that out.
Because the government hasn't been able to do anything right for 270 years, why do you think they're suddenly gonna wake up a figure out mass manufacturing?
We can't educate our kids at an acceptable level without billions of dollars being donated on top of all the tax collected, we can't figure out how to make medicare work responsibly despite literally being able to control costs, what do you think makes drug manufacturing any different?
In the US, one party has dedicated itself to making sure the government is dysfunctional for a _long_ time so that it can run on the platform that government doesn’t work and we should privatize everything. This is not a fact of nature, it’s a willful decision. For example, the US used to be a leader in education. The thing that changed since then is one party started defunding education and moving that money to private prisons and defense.
If we as a people collectively agreed that we are as smart as other countries, there’s no reason we can’t have a functional government that can handle public education and vaccine efforts and keep us safe and maintain our infrastructure and everything else we expect our government to do for us.
If your statement was true, Chicago and California would be bastions of government efficiency and capability. Instead we see both Republican and Democratic cities do terribly on most measures, and those cities that generally prosper have very little to do with who is in control other than it not being a single party and they have the right conditions for job growth.
School funding happens at the state level too, not just the federal grants.
It's funny you bring that up, because my comment originally even included a bit about how a lot of our current problems can be traced back to Reagan's presidency. He was previously governor of California. Guess when California stopped offering free higher education?
Chicago is in Illinois, which has had a lot of flip-flopping between red and blue governors and has an infamous history of governors going to jail for corruption.
Also I'm not claiming that Democrats haven't done shitty things. Daley bankrupted Chicago and privatized a lot of our public services while running as a Democrat and some of those jailed governors were democrats, but I do think the GOP is more homogeneous in its efforts to break down the government. I mean privatizing everything is a platform they openly campaign on!
If your claim that prosperity has nothing to do with who is in charge were true, we wouldn't see a pattern of blue states outperforming red states economically or a national pattern of economic growth after a democrat president and decline after a republican president.
Coincidentally, I live in Chicago and used to live in California. People love to use both places as punching bags when talking about national problems, despite one being a state and the other a city! It's different types/scales of problems.
Many cities have and are. It's worth pointing out that there are literally millions of Trump supporters here, and plenty of Republican politicians to boot. It's not like California is pure blue.
Plus, democrats are conservatives, so, it's not like they're automatically leftists just because they're blue.
No, there is not free public education anymore so in California than Texas.
> It's worth pointing out that there are literally millions of Trump supporters here
Don’t try to blame them. They have no power at the state and even the extremely Trump-devoid Bay Area (iirc <10% support) has failed to offer anything approximating a solution to housing or good education. The answer to shitty schools in the bay was a lottery to make sure everyone got to suffer the shit, rather than you know... fixing the shitty schools.
> Because the government hasn't been able to do anything right for 270 years, why do you think they're suddenly gonna wake up a figure out mass manufacturing?
worked just fine for penicillin during world war 2
The nominal world economy 'GDP' was $90T in 2019 [0]. An economic contraction of 5% because of the pandemic would mean a loss of $4500B. If a vaccine helps to avoid that, even a cost of dozens of billion dollars for it would be peanuts in comparison.
This is only the economic cost avoided let alone the human tragedies.
Edit: german Wikipedia suggest that the contraction is only expected to be 3% but because of the numbers involved even that doesn't really matter for the argument.
This is also how criminal mobs operate, in terms of protection money, extortion, ransom, etc. The underlying economic principle is the same ("gee, sure would be a shame if this expensive thing X were to break..."). Beware of relying on this as the only reason to justify the cost.
Hopefully there is some other significant differentiating characteristic or attribute to justify this state of affairs between society and big pharma, that would distinguish it from the same analysis you would use to pay a ransom or protection fee.
We are talking about a company providing a service. They might not have invented the vaccine but they are providing the means to bring it from proof of concept into mass production. The commenter seemed to think that this isn't worth money.
It's not an "argument" per se, as in whether we should or shouldn't pay the pharma companies. Of course we should pay pharma for this for COVID, and of course it is "worth it." There is no argument (from me at least) about that tactical decision.
My larger point is that for-profit pharma/healthcare is not a healthy marketplace (... or at best, it's an immature one). In the not-so-distant past (in America, up until the Civil War or thereabouts), firefighting was mostly privatized (meaning not government-run) [0], and brigades would compete (literally sometimes fighting in the streets, covering the hydrant to impede rival brigades, etc.) to claim the prize of the insurance payout for saving a building [1], which doesn't really serve the interests of the victims of fires.
I think the incentives of for-profit firefighters are not all that dissimilar from the incentives of modern pharma companies today (i.e. pay us to save your building from this fire, vs pay us to research this vaccine), and I would hope to evolve this pharma industry and this marketplace (of "demand" for life/health, vs "supply" of pharma research and resources) into something more mature and with fewer perverse incentives in the long-run.
I was not familiar with the history of firefighting until now and this is pretty wild. Thank you for clarifying what you meant with your earlier comment. I agree that for-profit healthcare and pharma is a huge problem, exactly because of the misaligned incentives for companies and patients.
The question is not if it’s valuable, the question is if it’s subsided. Farmers producing corn add some value to the process, but in western countries ~100% of their profits are from government subsidies. This does incentivize them to be more efficient, but it also means their constantly looking for a larger handout.
In the case of farm subsidies it’s grown to the point of being actively unhealthy both in economic terms and the actual root cause of the obesity epidemic. Without sufficient calories you can’t have an obese population due to physics. Medical subsidies have resulted in a host of related problems not just in economic costs, but also in what research gets done and how efficient that is.
The cost of Medical studies in the US has grown wildly out of proportion because their a profit center. This perversely slows down the rate of medical research, even in the case of emergencies like covid 19.
You don’t get a significant percentage of the population to obese in a famine. Simply maintaining obesity across over 40% of the population takes a lot of energy, let alone morbid obesity numbers.
Yes you certainly can. Famines are not spread equally. The people that can afford to have food shipped in (i.e. anyone who can afford to order things on Amazon) could comfortably remain fat while the entire lower class in their local area suffered from a famine.
Having food shipped in still requires it to be created somewhere to be shipped out.
It’s very possible for some percentage of the population to starve even during a food surplus, but starving people will bid up the cost of food to the point where you can’t get a 40% of the population to have a surplus in a famine in any society that we know about.
Here is the official definition for the minimum to qualify as a famine:
“At least 20% of households in an area face extreme food shortages with a limited ability to cope
The prevalence of acute malnutrition in children exceeds 30%
The death rate exceeds two people per 10,000 people per day“
That’s killing off over 7% of the population per year.
citation? That seems very unlikely. US farmers constantly look for greater efficiencies. They are also among the most conservative about land policy i.e. erosion, chemical application etc because it costs them money.
On average your looking at ~90B in net profits from farming, the subsidies however are much harder to track down. Ethanol subsides for example are often excluded as are insurance, tariffs etc.
Ahh, no it simply wasn’t clear what you where asking about.
There are a lot of ways to slice this up. “Overall agricultural subsidies in 2010 were estimated at $172 billion by a European agricultural industry association; however, the majority of this estimate consists of food stamps and other consumer subsidies, so it is not comparable to the 2005 estimate.” https://en.wikipedia.org/wiki/Agricultural_subsidy#United_St...
One example of this is Americans for example pay 3 billion dollars more for sugar than international market rates. But, only a fraction of that directly ends up in farmers pockets. You can either take the full 3 billion as a government subsidy or exclude most of it. Similarly, propaganda and what’s allowed in food lunch programs gets tricky.
So, I am not endorsing any specific estimate, just saying the total industry profits are approximately the same as the total subsidy. Add up just direct federal subsidies gets you lower numbers especially if you try an exclude state, ethanol, R&D, loans, Education, tax breaks, and other less obvious handouts.
PS: Silly me, I forgot about all the little exceptions in environmental, immigration, labor laws, use of federal lands, etc.
You missed the point that we already paid for the development of this vaccine by paying taxes. We should now only pay for the production, not for the intellectual property rights.
OR we could look at it as if the pandemic has already cost us 4.5T based on your figures, and that's enough. We come together and defeat the virus without anyone profiting - we all lose, we've all lost already, ffs, let's let people profit off of the death, because why not?
If "we" gave you $20B to move a vaccine from proof-of-concept to production, could you do it? I know I couldn't... That's a service, it's worth money, it's worth paying for.
Edit: people don't seem to understand that there are several stages in pharma development... (1) research, (2) trials, (3) scaling production. It sounds to me that even if (1) and (2) are "paid for" (with public money), (3) is still non-trivial and therefore expensive.
No one is claiming otherwise. And back to normal is still a long ways off.
If you’re admitting we’re giving them money for a thing, it’s paid for. I don’t know why you quote it like that, transfer payments of public money to private institutions is a thing, is it up for debate it happens?
Also cost is emotional. Does it have to be 20 billion or is the government handing out cheddar for consulting jobs later?
There’s more too it than high school capitalist theory. Just because you can’t for $20 billion doesn’t mean someone else couldn’t for $5.
But we hide the work in private accounts. Humanities work, built towards by countless hands and minds.
Yeah ok we get it, Murray Rothbard; You’re only 1 in 7 billion. Why does your theory matter? Roll up them sleeves. What? He’s dead? In the bin with it, no need to carry water for a dead man.
No, we're only paying for part of 'it'. The cure isn't just research, it's also logistics and there does not exist a capable non-profit to do the logistics part of it in such a short time. Also you underestimate how much it costs to build such a supply chain capable of producing and shipping that many vaccines around the world. Hint: the research costs are just a fraction of the logistics cost, you just don't see that up front because it's also used to ship other stuff besides vaccines.
These things cost money, and you assume your taxes are covering them in full. They don't.
I think the key desire is that the intellectual property, built from publicly funded research, should not be owned by a single corporation. Production and distribution are of tremendous value and these companies should be rewarded for providing that value. But the vaccine itself? Why not let others invest capital and try to produce & distribute the vaccine?
especially to the shareholders ... holding shares and getting dividends (and no, for a 100 year old company these people didn't invest at all in the business case. They invested in a financial product.)
You don't get it. Developing vaccines is nothing like making cars. Our understanding of how the human body works is comical compared to our understanding of materials science and engineering, design and other aspects of making cars.
Developing vaccines is a long, treacherous journey on a narrow ledge with cliffs on either side from start to finish. Infectious diseases research has seen a sharp decline in funding and commercial interest in general. Because of how little we know about the body, most research doesn't generate results that can be turned into money. The only way to continue to support research is via public funds and grants. The public funding of science has been a major contributing factor for our advancements in this kind of research.
How is this any different than a government bond program meant to finance the projects? Whether the profit is derived via increased stock price, or derived from interest paid by the government directly through taxes, how is it fundamentally different? The government can't typically just print money (to keep the economy okay). It has to either derive tax to get the funds, or borrow, which again privatizes the profit (in the form of interest).
Would you rather hold on to your anti-corporate principles or have a safe and effective vaccine to protect the most vulnerable in the world? These public-private partnerships aren't ideal, but there hasn't been any other way in history to develop safe vaccines on such short timeline.
> Who cares. I'd gladly give this company a couple of billion if it means they can get us back to normal.
This kind of thinking is worrisome to me. It sets a horrible precedent. Previously in times of war private business would be forced into helping the people fight a common enemy. These days a war on a virus has zero help from business and they essentially have a position of power to sit on their hands taking billions of public subsidy and then take the people's money and effort for their own.
Why do we take this with such apathy? Why is it that a country run by the people for the people has no power in the populace hands? We are doing everything we can to help, committing billions of dollars which represents millions of hours of public production to solve a problem that CEOs only want to assist in if they can up their share price.
Since we care so much about our health and the health of loved ones why have we not used these unprecedented times to reform the healthcare industry?
We are paying twice for this. Once to fund the research, which we then give away, and then again for the manufacture and distribution which is priced as if the pharma did all the research. These vaccines are going to cost anywhere between $15 and $37 a shot. You cannot tell me that's how much these vaccines cost to make in quantity. Why is there any profit at all? Let's get ourselves out of this shit without encumbering any more debt on top of an economy that is already falling into a black hole.
This stuff is morally corrupt, and to say 'who cares' makes me sad. We should care, maybe we accept the shit we have, but we should care about it. This stuff should be criticized, we should use our agency to change what is wrong, not to support it.
Every day I fear we are all fucked. This sort of thinking is why we deserve the likes of Trump and Boris. We bring this crap on ourselves and then moan about it.
You talk about getting back to 'normal', well we slowly sold normal. These decisions do not have zero impact on the future, they affirm a shitty attitude and set the path for future generations who won't know any better.
Do you think that the more profit available to pharma, the more capable the workers attracted to the field will be? And therefore the faster results will be achieved? I don’t mean just the bench scientists, but all the other people - programmers, lawyers, managers, fabrication engineers, supply chain ops, etc - required to take an idea from paper to mass production. Having worked in biotech startups myself I understand how inefficient the current system is, but at the same time I can’t foresee a better one.
None of this speaks to the social cancer that is corporations draining the society they function in. Individuals are expected to sacrifice and pull together, do the research, finance pharma production, give away patents, and yet the big pharmaceutical sits back and drains all of this into their stock. It's just not right.
Let them make a profit when we are thriving not while everyone else is suffering and making sacrifices.
Just because they hold the patent doesn't mean they won't license it out. We're talking about the entire world here.
I know a lot of people, Americans in particular, are weary of 'big pharma' and for-profit healthcare. And Americans have good reason for that mistrust. But this isn't just an American issue.
Other governments such as the EU and India will force their hand if needed for the public good. As they've done countless times in the past. We just need to get this developed and manufactured as fast as possible.
And the linked article said the clash was between this pharmaceutical behemoth or a startup from the university. I'll take the behemoth now.
"The scientists’ small biotech company—a spinout partially funded by Oxford—was refusing to hand over intellectual-property rights. To outflank their bosses, the scientists asked a London investment banker to help explore other potential deals."
The patent protects from somebody simply copying the formula. Which is many orders of magnitude cheaper than doing research and development, especially on human subjects.
Trials and regulatory approvals are a huge cost too.
If the government paid for all of that (including opportunity costs + a decent margin), then the government should have asked for the patent rights (or at least a commitment on pricing).
Has any serious journalist looked into exactly what the world governments paid for and exactly what the deals with the drug companies look like?
All I can find are biased opinion pieces devoid of actual information.
The FT had some coverage of this, but it wasn't massively in depth. The one thing I remember is that the AZ would be sold without profit until the end of the pandemic, which was contractually defined as June 2021.
Incidentally, if you want serious journalism, the FT is worth paying for.
But, for instance - public money is used to build roads, yet companies that build them make money in the process. There is no state-owned road building company. What's the difference here?
Public money pays for the roads. After the road is built, the road belongs to the public. Public money pays for the research. After the research finishes, the results should belong to the public, the same way as the road does.
> After the road is built, the road belongs to the public.
Depending on where you live, you could very well be under the impression that the roads belong to delivery companies, taxis, etc. (private companies that make money off them) as they are effectively useless to everyone else (= the public) while they are constantly blocking them.
That’s a faulty parallel. The road belongs to the public, while only the building is tendered to a private (in a presumably competitive market) to maximize quality and price ratio.
In this case the building is publicly funded for a profit AND the final result donated in “perpetuity” to make it a private TOLL road.
Double dip?
(I’m ok with subsidizing the research, and even negotiating a bulk manufacturing contract with an agreed margin... but a patent? Isn’t that bending too far?)
My village has their own road building and repairing department--mostly used for repairing. It's called the department of public works. We have our own utility company too. Both of those end up being cheaper than the having private companies do it.
In what way? Yes, the taxes paid for research, then taxes paid to purchase the product. But if everything was state owned top to bottom, the taxes would have had to fund research, then manufacturing, production and distribution. I wager the amount of money spent would have been exactly the same, so it's more like an accounting trick than an actual difference.
Its not about manufacturing costs. The companies continue to own the patents and after some period of time have every plan to start charging for use of it. This means they can get rich for decades off of the taxpayer-funded research. Meanwhile the governments have agreed to take on the risk by buying tens of millions of doses before they vaccines are even approved which means some of them will likely be waste due to either not getting approval or coming after more effective drugs.
Socialized risk and privatized profits. A capitalist's dream.
To go back to your highway analogy, its as if the government contracted for the entire interstate highway system to be built and then let various private companies charge a perpetual toll to use the roads in addition to the money they made for building it.
Its not an accounting trick, its a perpetual royalty on the taxpayer's expense if the drug works (and a profit even if their drug never passes Phase 3 clinical trials).
Is another state going to get sued for having a different company build a road of the same material? I dunno, maybe Asphalt Co should be getting license fees for every road built. Maybe even add a toll booth so drivers have to pay a license fee to Asphalt Co to drive on their roads
Noam Chomsky has quite a bone to pick about toll roads
There's no(t necessarily a) question of any non-profit startup there. The problem is that the people who paid for the development of the product should also hold rights over the product. If the vaccine was developed with public money, it should be publicly available -- not necessarily (but yes, also to) non-profit startups, but also to any other manufacturer in the pharmaceutical industry, since they (allegedly, in any case...) pay taxes, too, and have therefore invested in this product.
If Merck wants to use their proven manufacturing base with an excellent delivery track record (which nobody is denying, after all), that's great. They can:
1. Put their money into the development of said vaccine, or
2. Acquire the license to manufacture it, at a reasonable price, like they do with any technology that wasn't developed using public money, or
3. If we don't want stuff that's already been paid for with public money to be sold to manufacturers, which I don't disagree with at all, then, sure, they should get it for free -- but in that case they shouldn't be the sole owner of the rights towards that product, either.
(Edit: FWIW, I'm all for 3. I've worked in the medical industry and I know full well that there's a great deal of work that goes between first-stage research and final production, and that it's incredibly hard and expensive to take the result of a publicly-funded research program and turn it into a product. That doesn't change the fact that said research programs are publicly-funded -- their results should be available to anyone who paid for them. If someone wants exclusive rights to the result of some research program, then they're welcome to pay for it themselves.)
As it stands now, they own the rights (including licensing rights!) to a bunch of products that they haven't paid for at all.
All the suits blabber on and on and on about how the government should keep its nose out of their business. How about they tell the government where to stick it when it's about paying for their research, too?
Then it needs to be a cost-plus model. They should absolutely be able to make a profit for manufacturing and handling logistics. They shouldn't be making a 4000% profit when "we" collectively funded all the research.
The possibility of them 'being able to do that' is because of laws that got passed by democratically elected officials.
If you don't like that, vote someone in power who regulates that more.
The problem with these discussions is that nobody tells their opinions to their representative, they just blurt it out into the 'aether' on a rando internet forum.
True change starts with calling your representative. If they don't do what you ask them to, then have other people ask as well. Finally, have them vote them out of office if a sufficient ammount of people want the same thing that the representative won't do (eg. represent their constituents).
>If you don't like that, vote someone in power who regulates that more.
That's an awful lot of assumptions on your part. I have voted out someone who didn't represent these values in exchange for someone who does. I don't need to contact my representative on this specific issue because I already know where she stands, but if we were in disagreement I would (and have).
Posting about it on the internet is to garner additional support and discussion... you know the entire reason HN exists?
I care. I care that we look past the end of our nose for public health to give the Saulks of the world a chance and let the billionaires grab some fucking pine.
They don't need the patent in order manufacture the vaccine. Only allowing one company to manufacture the vaccine (or to control who manufactures the vaccine) will likely rise prices.
I mean, I would gladly give companies a couple of billions if it means people stop panicking and we all can start living again. The vaccine doesn't even have to actually work.
The United States Military has the best logistics system in the world. I'd rather have them handle manufacturing and rollout than either a multinational or a startup.
Could you please indicate where you heard that Merck has any ownership of the patents to the Oxford vaccine? The cited article indicates that it’s is AstraZeneca who have done a deal with Oxford and that the deal with Merch, while an early option, fell though.
Is would seem “US BigParma” are not involved, as AstraZeneca is a British/Swedish company.
yeah it is just how the world we live in now days works. Most people don't know who owns what!
For example, Russians owns a bunch of funds in US mutual funds, and us big oil owns a lot stakes in Russian oils. So the whole idea that we are still living in the idea of nation state is over! Private company (like Federal reserve) has their own military.
Most things are hidden behind attorney-client privilege and ran by a hand full of law-firms for the elite rich people. Someone who have managed billions dollars for the public and private sector has once said no body really know who owns the debt of the planet.
Personally I support more transparency let everything come out and let the people judge. There is the risk of anger of mop and chopping off some heads like the French did. Truth will set you free, at first if fucking piss you off. Hope everyone will exercise some constrains and respect the due process even for those who have done so much bad things.
According to that article Merck got cut out of the deal and Oxford will get 6% royalties on the vaccine, from a UK/Swedish outfit. So nothing to do with US big pharma and Oxford will get upwards of £100m. It’s not is if they’d have got nothing out of the Merck deal either.
This is very disappointing. A lot of people are posting on this thread based on this misinformation.
The story appears to tell exactly the opposite of your comment : Merck failed to do a deal because Oxford held out for public good outcomes that Merck wouldn't meet, and AZ did.
it seems more like a collaboration. the private sector doesnt have the money or incentive to do such a thing (at an individual business level) but they have the ability to execute on it if incentivized.
the public sector doesnt have the agility or flexibility to do such a thing but they definitely have the money and incentives to make it happen.
the two combine to create a big, powerful, fast-moving machine that solves a problem.
Someone is going to pay. It may not be you at the point of the needle, but somebody will.
Governments will pay a lot to get their economies going again. That burden will in turn fall on taxpayers one way or another; whether it's directly via taxes or budget cuts or indirectly via inflation or debt service.
Yes, I realize that. My comment was in response to the criticism of these companies being funded by tax dollars while being granted a patent. The implication being that we're paying (as taxpayers) but getting nothing in return since we would have to pay for the vaccine anyway.
My response is that we're getting the vaccine for free in return.
That said, I'm not sure that it's actually going to be free. That's just what I heard. I should point that out - I don't want to propagate bad info.
What you get in return is somebody (the government) took the risk of a blind faith payment to have a university develop a vaccine.
That's what you paid for, not for production, not for distribution, not for anything else.
You didn't pay taxes for a free vaccine, because you don't pay remotely enough taxes for that to be viable at all. Unless every country on earth takes their fair share of blind-faith financing a single company.
My understanding is that because stimulus packages are good for the stock market. When hopes are up about a vaccine, the possibility of a stimulus drops, hence the market comes down.
I've only been following the market for about a year, but its a weird thing.
The word jab is standard UK English for 'shot'. It might be slightly informal, but it's definitely standard to see it in the news and in government publications.
Admit it, you're just subconciously afraid of needles as most people.
Noticed it with Trump. No way he'd take an experimental COVID vaccine, but an experimental antibody drug cocktail through the mouth was more than ok to him.
Pro tip: it all ends up in the bloodstream in the end.
They don't release more details officially due to patient confidentiality, but the unofficial word was that a young doctor treating COVID patients died of COVID during the trial, but was in the control group and did not receive the vaccine. It is very sad whenever a doctor dies trying to save others, but especially because they may still be alive if they had been randomized to the vaccination group (of course we don't know that for sure though, since the vaccine may still prove to be effective or ineffective).
What has been reported in the local media, is that the doctor who died did not get the vaccine. He was one of the test subjects, but half of the test subjects receive a placebo instead of the vaccine (the whole point of the experiment is to see how the vaccine compares with a placebo); he was in the group that received the placebo.
Bet you they give it to everyone for free everywhere in the world except for the USA, where they charge 600 dollars a dose and consequently we never reach herd immunity and have endemic Covid indefinitely.
Would you please stop posting flamebait to HN and not use the site primarily for ideological battle? We ban accounts that do those things and have already had to ask you a few times.
Does this comment really read as flamebait? The article is about vaccines. A vaccine has to be administered to everyone to work. But I’m very skeptical that it’s actually going to happen given the way our medical system works here. So, I predict that there’s a good chance we won’t get herd immunity. I just don’t see how that’s flamebait. It’s more, known facts and extrapolation.
Sure it does. This may be a case of "comments in the rear view mirror are much larger than they appear", i.e. people underestimate how provocative their posts are.
US healthcare differences are a classic flamewar topic and nationalistic flamewar is particularly ugly and pointless. Your comment wasn't thoughtful/substantive, it was snarky/hyperbolic. Ergo flamebait.
You can look up the moderator commentary on 'facts' and flamebait (tldr is, you can flamebait with facts) but these aren't even facts - free vaccine has been the stated official plan in the US for months.
800 for the dose, 300 for a list of other things on the bill, and you're required by law to get the injection today. if you can't afford it, that's prison time, where you'll get the vaccinee but also need to work for the bill, probably producing maga-caps or substituting sick/dead medical personnel.
Given that immunity from infection is currently questionable your suggestion doesn't make sense. The reason the findings mentioned in this article are important is because the immune response seems to be stronger than that seen in people that have been infected and recovered. So this vaccine would be better at creating herd immunity than just allowing everyone to get infected. At the same time vaccinations will have a reduced impact on people than actually catching the virus would.
There is a difference between the level of illness experienced by those who are vaccinated Vs those who get infected, so more old people will die as a result of infection than would die as a result of vaccination.
So no, it would not be better for healthy adults and kids to get it in Q2 2020. Also how do you propose that you only infect the healthy adults and kids?
How is immunity from infection questionable? We had 43 million cases and about a dozen or so reinfections. Not sure if confirmed reinfections reach the double digits yet.
So studies of other coronaviruses show immunity lasted 6-12 months. We’re a but early to see mass reinfections.
That said, my guess would be normal reinfections would be less severe, more like a cold. There have been some severe reinfections but any reinfection under six months suggests something atypical in the immune response.
Also SARS-Cov-1 produced a longer immune response so that may happen here.
But lifelong sterilizing immunity seems pretty unlikely based on what we know so far. The vaccines aren’t aiming at sterilizing immunity actually, their goal is to greatly lower the severity of the infection.
Read the papers on it, antibody tests in people who have previously tested positive for covid have found little or no antibodies in tests taken 3 months after infection. So it appears as if there is a limited/short term immunity after initial infection. The vaccine appears to produce a much stronger immune response, such that antibodies can be identified in tests some time after the vaccination.
You can get limited immunity from the common cold after being infected but you are just as likely to catch it 12 months later anyway. With covid that means we are dealing with it annually, which our health services cannot keep up with.
There are more immune mechanizms beside antibodies (T-cells, B-cells).
For the common cold there are different viruses, so you may get a cold caused by different ones.
antibodies disapear quickly, but the B-memory cells that produce them are still in the body ready to be mobilized.
"Common cold" and "flu" is not 1 virus, but hundreds of different viruses which is why you get them repeatedly. You do build immunity though. It's why children always have a cold and adults a lot less common.
We don't know if it does yet. We know it causes an immune response. We don't know if that stops you from catching it, and we don't know if it stops you from being infectious. It tips the scales in that direction, and all we really need is for it to be effective enough to drop R0 low enough that coupling it with reasonable restrictions makes the virus go away, which is why it's worth pursuing, but that's a different goal to ensuring you can't catch it at all.
> Wouldn't it have been better if healthy kids and adults caught it in q2 2020?
No.
We have one population. There's no way to segment it to allow people at low risk to catch the virus without also allowing people at high risk to get it.
It’s super easy to make those decisions as an abstract mathematical problem. It is another when someone puts your family in front of you and asks you to roll the dice.
As an abstract mathematical problem if somehow herd immunity could be achieved without a vaccine then it sounds like a fine idea. The fact is that immunity after infection does not last long enough to achieve significant enough immunity to get to a useful herd immunity. This of course is what all the medical experts understand which is why Europe is going through lockdowns and Putin has been hiding in a bunker. There have been strict lockdowns in China and most other major governments have taken some sort of similar response, even Sweden eventually. There is almost nothing all of these governments have ever agreed on so universally.
Don’t expect a reply justifying my comment on HN with robust data, I have better things to do with my time like play in a park.
That option was apparently actively considered by the UK Government's scientific advisory group, but rejected on the basis that it would not actually be possible to prevent transmission from less-vulnerable groups to more-vulnerable groups. Reference: https://archive.is/43ir5
The implication that we even slowed the trajectory isn't well established. It's likely, but not proven. Let's not get ahead of ourselves by pretending there's evidence millions would have died when there's not even a strong correlation between mandates (as defined by the Oxford stringency index database) and reduced death.
and nowhere that I'm aware of came close to running out of ventilators. New York, one of the hardest hit places in the world may have used a third of their available ventilators. They used around 1/2 of the ventilators they reported available to them in 2015 so it wasn't even close to being the limiting factor in healthcare.
> If we let everyone get it in Q2 2020, millions would have died when we ran out of ventilators.
How do you explain countries like Belarus, Serbia and Sweden, or parts of the US like South Dakota, where no or very lax measures were taken but what you describe didn’t happen?
In fact, is there any evidence that this happened anywhere, or is it all just conjecture based on modeling?
Last I checked Sweden had 110k cases and 5.5k dead. That's an almost exactly 5% fatality rate. Compare that to neighbouring Denmark with 40k cases and 700 dead gives you a 1.75% fatality rate.
Seems to me that there is good basic evidence right there for Sweden's approach being much more deadly.
We can argue back and forth about the relative value of freedom vs lives or whether Denmark will ultimately have as many dead etc. But right now, it seems that controlling numbers saves lives...
Comparing the case fatality rates makes no sense unless you have the same ability to get a test in both countries. If one country were to test everyone, including asymptomatic people, then their CFR would be lower than a country with more limited testing, simply because the denominator would include those large number of minimally symptomatic or asymptomatic patients that would be missed in the other country.
Also, the CFR is likely intrinsic to the virus, modified slightly by patient population and type of medical care available (both of the latter are probably very similar between the two countries). So any differences in CFR between the two countries mostly reflects the testing issue.
If you do want to compare the two countries, then compare the per capita death rate from covid (assuming everyone who dies in both countries actually gets a covid test - that might not be the case for old people who die at home, where even in developed countries, their primary doctor will just issue a death certificate saying “old age” or “heart attack” in the absence of any information to the contrary. )
1. You cannot just rely on how many sick people happen to be tested. Every single serology study implies a IFR of well under one percent. I am willing to bet that it will end up between 0.1 and 0.6 % for any developed country.
2. You cherrypick your data if you compare Sweden with Denmark or Germany and not with France or the UK.
My hypothesis is that countries that protect the elderly, and especially nursing homes, well have much fewer deaths. In every country this is were the deaths are concentrated.
> This is a virus with bad long-term effects on the body.
In what percentage of people who get COVID-19 are there bad long-term effects? What other conditions did the people get bad long term effects have? How does these numbers compare with other diseases?
Damage to the heart, the brain, even for mild or asymptotic cases. My references are previous posts on HN or on phys.org as you can easily search it.
As you said there are scarce data yet, but the risks are scary. In these conditions, it's obvious one should avoid relying on a herd immunity induced by the virus.
By the way, between "relying on virus-induced herd immunity" and just keeping safe with mask and waiting for the vaccine to come, why the rush to get the virus??
There is a risk, there is the possibility to wait it over. So why just not do that and wait the safe solution?
Suicide, abuse/trauma, avoided medical treatments, drug and alcohol addictions, and depression have all been seen to increase since we first had lockdowns.
There is no safe solution, it's a decision between protecting the 0.5% old, obese, and sick or the 99.5%
> Suicide, abuse/trauma, [...], drug and alcohol addictions, and depression have all been seen to increase since we first had lockdowns.
Correlation versus causation.
We're in the middle of a major health emergency. Why are you attributing those to the effects of lockdowns, rather than the effects of the pandemic? You don't think that the risk to personal health of a potentially lethal virus, seeing older friends and relatives dying, and worrying about the risk of health systems collapsing are causing any of the above?
In March, someone I know in Italy passed on the virus to his grandfather, who died at home. All the ambulances in the area were tied up for hours. You can imagine the effect on his mental health. I doubt the impact was comparable to the effects of intermittent lockdowns.
A uk study suggests 12% have symptoms longer than 30 days. Beyond that, hard to say. We also don’t havea good measure of invisible damage: do survivors have reduced lung function from pneumonia? Damage to endothelium predisposing to pneumonia? Too soon to tell.
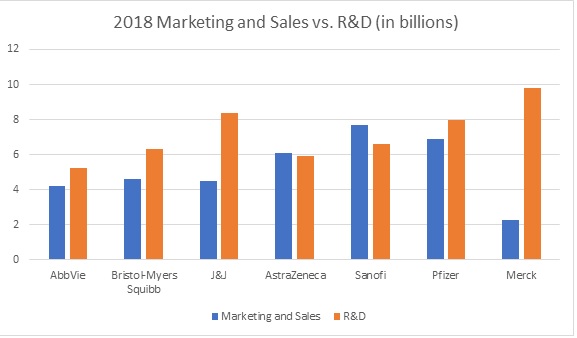{kind=link}
https://news.ycombinator.com/item?id=24894622&p=2