My ex-boyfriend was an attorney at UPMC doing M&A. Their business strategy goes something like this:
1. "Rescue" the only small hospital in a rural area through merger or acquisition. The hospital entity is a "non-profit."
2. Over the course of the next year or two ramp up sales of the very much for-profit (and, conveniently, affiliated) health insurance plan, UPMC Health Plan to all major local employers.
3. Once sales of the health insurance plan reach "critical mass" within the community, the "non-profit" hospital becomes out of network, and ridiculously expensive, for all major insurers except one: UPMC Health Plan.
4. Within the year all local employers are basically forced to adopt UPMC Health Plan.
5. UPMC Hospital and UPMC Health Plan rates go up. UPMC Health Plan shareholders rake in the money while a small town goes broke trying to receive adequate healthcare.
As someone who used to live in Pittsburgh - fuck UPMC. They may do some excellent research and have great doctors, but their business practices are akin to Comcast. So many hidden fees (some of which I suspect would be overturned if taken to court, but that would require a class action lawsuit or someone willing to spend 1000x on lawyers than paying the fees) and just terrible practices as you mentioned. They buy up real estate in bulk and then pay no taxes because they are a non-profit (something that is regularly challenged in court but they just threaten to leave the city they're named after). What's worse is many of the buildings they buy are historic, and they raze them and replace them with cookie-cutter corporate facilities. And as they raise prices and screw over customers their executive suite rake in 7 digit salaries. I believe that running an organization of this size should command large salaries, but they are doing it by fucking over their customers not by providing better healthcare. And since they're the largest employer in the state (and this is in Pennsylvania which includes Philadelphia) they just keep doing this shit.
Fuck UPMC. The only other non-profit organization I can think of that is so undeserving of the status is the NFL. We need stronger enforcement against entities that are clearly operating for a profit while reaping the benefits of paying no taxes.
MLB also doesn't deserve the antitrust exemption it has as a pure accident of judicial history, unlike all other sports leagues.
(The exemption was subsequently narrowed by Congress but not eliminated, which MLB effectively argues means they implicitly endorsed the remaining exemption and that any change would need to come from Congress. SCOTUS has upheld the exemption twice on the basis of "we don't want to disrupt things" and has refused reconsideration as recently as this year.)
Out here, it’s Sutter Health. They have a slightly different strategy involving acquiring near-monopoly status and screwing everyone over. It’s gotten so bad that the state is suing to partially break them up.
To be somewhat fair to the hospital groups in question, a lot of this is driven by outlandish regulation that makes it hard for independent medical groups to survive.
That regulation favors hospital groups and reinforces their monopolies. Independent physicians who can't deal with the regulations sell out to big hospital groups, who then, enabled by their greater control of physician supply, squeeze insurance companies, who then in turn must squeeze the remaining independent physicians who can't fight back, who then give up and sell to hospitals
I think in some ways the ACA empowered monopolies by enabling them to further consolidate physician supply in the guise of integrating data for "population health"
The ACA was essentially written by the big industry insiders that are now benefiting from it. This is cronyism, not capitalism, and is the hallmark of a socialist / regulatory state.
Sutter is pretty good though, it's nice to have comprehensive care in the same EMR. Kaiser is a competitor too and is actually the model the OP denigrates as UPMC at reasonable costs. Stanford is also very good especially if you actually get sick and need comprehensive care.
This is a business modell that works only because of the difficulty of opening a new small hospital. Lets remember that any market is subject to the mopolization of consolidation, its barriers to entry that make them sustainable.
Yep. Just to elaborate here: In order to open a new hospital in an area you need to acquire a 'certificate of need'[1]. You know who approves those certificates? The other hospitals in the area. Your competition literally gets to decide whether or not you can compete with them.
"Certificate of Need (C.O.N.) programs are aimed at restraining health care facility costs and facilitating coordinated planning of new services and facility construction ... The basic assumption underlying CON regulation is that excess capacity stemming from overbuilding of health care facilities results in health care price inflation."
Two paragraphs in and I need to stop reading this, I'm getting murderously furious.
Ya, it's kind of incredible. And it's equally incredible how few people seem to know about this. It'd be such an easy thing to fix, and it would substantially improve competition for hospital services. It's completely beyond me why this isn't getting changed.
I completely agree. If we had to pick one thing to change to lower healthcare costs in the US, this wouldn't be a bad choice. Hospital costs are by far the largest contributor to US healthcare expenditure at 30%, and when you add in physician costs (since they are increasingly owned by hospitals) that's almost 50% of cost
My sort of crazy theory is that there is a behind the scenes lobbying / media battle between pharma, the hospital lobby, and the insurance lobby and that this dictates a lot of the national conversation around healthcare. Because healthcare is so opaque and complex, and because there is so much political energy around healthcare, it is hard for the public to be informed about the facts so they just respond to emotionally driven narratives in the media. Right now pharma is public enemy number one so everyone complains about drug prices even though hospitals are probably just as bad if not worse. Both trade groups spend roughly the same on lobbying although hospitals probably have more "soft" political power bc they are major employers in pretty much every county
> My sort of crazy theory is that there is a behind the scenes lobbying / media battle between pharma, the hospital lobby, and the insurance lobby and that this dictates a lot of the national conversation around healthcare.
It's important to point out that the insurance companies have no cost-lowering incentives though. They have an incentive to deny claims, but their incentive is actually to increase industry-wide healthcare costs because as long as the cost increase also applies to their competitors, it allows them to raise prices and higher premiums means more vig.
They're also the ones strongly against some of the proposals that would actually reduce costs significantly, like catastrophic-only insurance that would have people paying out of pocket for routine non-emergent care and provide the incentive to compare prices.
Totally this too. I feel like someone should compile a list of non-partisan (i.e. no more and no less socialization), simple ways to incrementally improve healthcare:
- No more Certificates of Need.
- Don't force insurance companies to take a fixed percentage of revenue as profit so that they are actually incentivized to care about the cost of medicine.
- Expand the scope of procedures that nurse practitioners are allowed to do.
- Make residency / med school less restrictive and awful. There is no reason doctors need to be working insanely long shifts during residency. The only reason that they are is as a filter, to keep the supply low.
- Remove tax incentives for employer-provided healthcare. Replace with dollar-equivalent direct subsidies to personal health insurance purchases.
- Allow people to sell their own organs [1].
I'm sure there's lots more. But these are the ones that spring to my mind.
Price transparency. Require medical providers to publish a price list for every service they provide, then let there be Expedia for scheduled medical procedures.
> Don't force insurance companies to take a fixed percentage of revenue as profit so that they are actually incentivized to care about the cost of medicine.
This wouldn't really work. The nature of the insurance market is they predict how much it would cost at what probability and then add a percentage as a risk premium. If you lowered the risk premium in absolute dollars against the same level of risk and cost, nobody would provide insurance. If you lowered the cost of claims for the same absolute dollar amount of risk premium, more companies would provide insurance and the competition would reduce the absolute amount of the risk premium per customer back to the original percentage (which is based on risk-adjusted reward) of the now-smaller cost/risk -- which is what they're trying to prevent.
What you need is for people to be buying less insurance, i.e. insurance covers what it's supposed to -- losses greater than what you can afford -- rather than covering routine low and medium cost procedures and removing anyone's incentive to care about prices when choosing a provider.
> Price transparency. Require medical providers to publish a price list for every service they provide, then let there be Expedia for scheduled medical procedures.
For providers that service insurance companies, its impossible. The insurance decides what to charge.
Price transparency is important for functioning markets, but im unconvinced its a key piece of health service costs. First, it doesnt matter if the doctor charges 100 or 1000, if the insurance covers it. Second, most health-services that matter are insurance-based: its a cost after you got the disease, which changes the decisions you get: if you are on Anthem and get cancer and see cancer treatment is cheaper on Cigna, are you going to change the entire doctor panel that diagnosed you? (Which btw ,is a degrade of medical care).
The only person that could benefit from high provider price transparency is insurance companies, since then they can choose to keep or not keep providers in their network: but they already have full price transparency, they get all the claims.
> For providers that service insurance companies, its impossible. The insurance decides what to charge. First, it doesnt matter if the doctor charges 100 or 1000, if the insurance covers it.
That's a fair point -- so fix that. The insurance company wants to decide how much they'll pay, so let them, and let it be on the low side and then let there be lower cost plans that only pay 80% or 65% of even that cost. Then publish the price list and let the customer choose their provider and pay out of pocket any amount above what the insurance company pays. This deal where the customer pays the same amount no matter which provider they use is poison.
> Second, most health-services that matter are insurance-based: its a cost after you got the disease, which changes the decisions you get: if you are on Anthem and get cancer and see cancer treatment is cheaper on Cigna, are you going to change the entire doctor panel that diagnosed you? (Which btw ,is a degrade of medical care).
Which is another reason why they should stop doing that, and just have a list of services they cover and the amount they pay under your plan. Then you go wherever and get the service and pay the difference between the insurance coverage you bought and the price the provider charges. There should be no such thing as out-of-network. If someone else charges more and you're willing to pay the difference, there you go.
> Price transparency. Require medical providers to publish a price list for every service they provide, then let there be Expedia for scheduled medical procedures.
Good one.
> This wouldn't really work. The nature of the insurance market is they predict how much it would cost at what probability and then add a percentage as a risk premium. If you lowered the risk premium in absolute dollars against the same level of risk and cost, nobody would provide insurance. If you lowered the cost of claims for the same absolute dollar amount of risk premium, more companies would provide insurance and the competition would reduce the absolute amount of the risk premium per customer back to the original percentage (which is based on risk-adjusted reward) of the now-smaller cost/risk -- which is what they're trying to prevent.
Hmmm...that's an interesting point. You might be right. However, it would incentivize them to control costs that are in some way unique to them. In other words, it'd incentivize them to negotiate deals with providers, or incentivize their customers to reduce their spending. Because while it is true that the equilibrium is the same level of profit for them, in the shorter run, each incremental unit of downward price movement they get within their own customer base is valuable to them. But I definitely agree my point here isn't as strong as I thought it was, thanks.
> What you need is for people to be buying less insurance, i.e. insurance covers what it's supposed to -- losses greater than what you can afford -- rather than covering routine low and medium cost procedures and removing anyone's incentive to care about prices when choosing a provider.
Ya, totally agree here too. I was just contemplating the fact that I pursue this exact strategy for my own insurance...when I pay for it out of pocket. My employer provides health insurance, so I choose the platinum-plated super deluxe package, and pay only a bit of the cost myself. For my car insurance, which I pay for on my own...I pay for the financially correct amount of insurance: insurance against ruin. I want to be insured against an unexpected cost that would financially ruin me...and aside from that, i'm happy to eat the costs of random fender benders myself, and rely on my own driving habits to minimize those costs.
>My sort of crazy theory is that there is a behind the scenes lobbying / media battle between pharma, the hospital lobby, and the insurance lobby and that this dictates a lot of the national conversation around healthcare.
Of course pharma, hospitals, and insurance are a major force on the right. But there's another culprit exerting force on the left that I rarely see discussed.
The nurses' union (National Nurses United) is TREMENDOUSLY powerful. I've been personally involved in several political races where their political machine was a decisive factor in delivering turnout, possibly more than any other union. Another advantage is that it tends to fly way under the radar of most union critics -- no one wants to criticize nurses, of all people. This, without a doubt, causes a chilling effect on Democratic politicians' willingness to write legislation that will threaten hospitals.
I suspect that FAR more people are paying for prescription pharma than are visiting hospitals. So, it's not totally irrational that pharma is perceived as a greater "enemy" than hospitals even given possibly equivalent price inflation.
Pharmaceuticals represent about 10% of healthcare spending for Americans. Inpatient and outpatient comes out to around 52% of annual healthcare costs.[0-1] While there are many issues in the pharmaceutical industry, as a whole I think they get an unnecessarily bad rap. Most of America's healthcare problems are self inflicted. There are a lot of things that need to be adjusted in order to let markets run effectively.
The US is actually middle-of-the-pack compared to other OECD countries in terms of rx drug spend as a percent of total healthcare costs. So while drugs are more expensive in the US, that's mostly just due to overall higher US healthcare costs, not because there's anything special about pharma in the US.
I know other countries spend more than the US on primary / preventative care (though dont have a source offhand); would be interested to know whether hospital spend as % of national HC spend is higher in the US (ive seen data suggesting that cost of a hospital bed for one night in the US is significantly higher than other OECD countries, but don't recall by how much)
That makes sense that more people spending money on drugs means it is a bigger focus for the public. However i'd strongly question the assumption that hospitals have less price inflation than drugs -- i think that the fact that we give hospitals the benefit of the doubt while blaming drug companies and insurers is a big part of the problem. The fact that far more people pay for rx drugs than hospital visits, yet hospital visits account for 3x as much spend, seems to me to be another data point suggesting we should focus more on hospital costs and less on drug costs
Air medical transport is only necessary in an emergency, at which point the customer needs it suddenly and has no opportunity to compare prices or refuse service.
This is exactly the market failure that causes municipal fire departments to exist, and should be solved in the same way, potentially by just having the fire department own and operate the helicopter(s).
It's bananas that emergency medical services like air transport can be "in network" and "out of network." As if the patient in need of services has the capacity or ability to control which helicopter comes to pick them up from their near-death experience.
At the Federal level it's really Medicare certification that is the stumbling block. Federal certificate of need laws were repealed in the 1980s, shortly after they were first tried.
States that don't have CON laws don't particularly have lower healthcare costs than states that do have them.
Most populated states have an overage of hospital beds, and anywhere from 40-50% of hospital revenues are from Medicare and 12-16% from Medicaid.
It’s pretty obvious when you visit a hospital, very few younger patients are hospitalized. Private insurance makes it very difficult to remain as an inpatient... even a major surgery like a spinal fusion is a 48 hour stay.
These institutions are mostly unnecessary and only exist because of their political power and government funding. There are exceptions, especially in rural areas and places in the south where the population of old people has boomed.
Insurance and public payers have pushed to make more care outpatient or delivered at less intensive facilities.
Occupancy rates have declined even as the number of licensed beds has gone down (with population increasing substantially, so the per capita effect is even bigger):
Especially look at small hospitals, which Medicare pays using a different formula to help keep them open (which isn't a bad thing, it increases access to care for lots of people).
This business model would have a problem with Maryland's all-payer system—hospitals are only allowed one price list; they can't give any individual insurer their own schedule.
Of course, being a reasonable idea means it's illegal; Maryland is currently the only state the feds allow to do this, so even if Harrisburg were willing they'd need to go through Washington.
A former employer was a smaller not for profit system. They made money but it was nothing like what the corporate hospital companies could do. The place eventually went bankrupt and was purchased by one of the bigger companies. No winners here except the large company.
The price gouging here comes from owning the only hospital that serves a particular area, not from any sort of evil government insurance mandate. Your choices are:
a) pay high prices at the door of the hospital
b) pay high insurance prices (to the same entity that owns the hospital)
I would be interested in a map that details distance to a major hospital vs price and also whether 95% of customers would be better served by air ambulance to the major hospital vs the local one.
One example is the hospital in El Granada just outside of Half Moon Bay. This hospital serves the local community yet it is only 30-45 mins over the hill to get to Stanford or Burlingame by car and less by helicopter. Considering that, the hospital is under utilized. Even further south in Pescardero you would go up to Stanford via La Honda typically. That is at the limit of the golden hour though. So here you have an example of a hospital that doesn't really need to exist except for widow maker events where you need to be seen as fast as possible (within the golden hour). So one question is, can you have smaller hospitals with lower revenues to serve this market. Even in rural hospitals if you need specialist care you will be transported out or otherwise wait several hours.
Could you argue that, with UPMC owning the hospital and also offering the best insurance plan for the area, the mandate increases the number of people buying their plan who otherwise would not?
> evil government insurance mandate
Don't try to gin us up. Honestly, I'd prefer single-payer. The stop-gap insurance mandate is far from optimal, which is why a lot of us don't like it - not because we think it's "evil."
I'm not super knowledgable about healthcare but my gut feeling says that this problem was around before government mandated insurance. I would think it would mitigate it a little but then also create the problem of uninsured people so I don't really follow how it makes the system better.
About 10 years ago I was able to buy individual family health insurance coverage for a reasonable cost. It excluded a couple of key things, such as maternity coverage, which I didn't need anyway, and certain pre-existing conditions which I didn't have, so I was OK with that.
You can't buy a plan like that now, because of mandated coverage of things that not everyone needs.
Costs of insurance where rising steadily and faster before the ACA. Since the ACA has started to take effect, the speed with which the cost of insurance rises has slowed.
While this plan you had ten years ago may have worked for you, many more people were paying out for low-cost plans that covered little, if anything. Mandated coverage isn't the perfect fit for everyone but, in my opinion, it is an improvement.
The ACA market place is supposed to reduce those costs.. The competition for patients by the insurance carriers who then negotiate rates with hospitals etc... Having more customers is not a prelude to higher prices. So your argument is bogus.
> The ACA market place is supposed to reduce those costs
Except it didn't and I question whether it was even supposed to. Costs were known to go up, they just mandated discounts for some types of consumers. There is no provider negotiation because the laws targeted the demand side and forced requirements upon them (consumers and insurers) and left the supply side unchecked (providers).
> Having more customers is not a prelude to higher prices.
Having more customers using your insurance is going to raise prices. The argument is not bogus.
Costs increased slower under Obama then the previous administration.
"..the average premium for single coverage through employers has gone up 28 percent “under Obama” That’s right again, but much lower than the growth of individual premiums during Bush’s first six years. That increase was 72 percent."
In that case wouldn't the alternative be having no insurance at all? How would that help?
Edit: I'm taking "government mandated third party payer" to mean something like the ACA mandate. If you meant a government mandated monopoly, then yes that's a terrible idea
The economics associated with modern healthcare demand consolidation, which basically means local cartels or monopolies for hospitals and health networks.
New medical schools must be allowed by the American Medical Association, artificially capping the number of doctors minted. This is why it's so difficult to get into medical school - the supply of spaces is constrained, unlike law school, where there is a spot for everyone who applies.
If we want to fix the medical and legal professions, and by fix I mean make it cheaper, we need to remove the warped incentives caused by the government that prevent natural competition from fixing the issues.
New medical schools have been established. The AMA doesn't cap the number of doctors minted. The actual cap is imposed by the number of residency slots that the government funds.
Residency slots don't have to be funded by the government.
I mean, it's reasonable to expect hospitals left to their own devices to fund the most profitable number of slots, so government is left to do the sensible thing for society in general, but health care providers have lots and lots of the money.
I think a tiny revenue tax would be a good way to fund slots. And structural incentives to host programs.
I agree. I don't know why Bill Gates, Bezos, Buffet and the rest of them don't fund residency spots... at least for 15 years. It would make a big difference in reducing costs. It's also easy to do.. just endow a medical school or hospital or something..
I see what you're saying there, but I'm not positive artificially capping the number of doctors minted is a terrible idea. Don't we want to make sure only the best and brightest end up being doctors? If there's a spot for everyone who applies to med school, wouldn't that leave us with far more incompetent doctors?
There should probably be more doctors, but it doesn't seem wise to lower the bar too far down.
This is the same broken logic as people who think they need to go to the "world's best X doctor" for care. That inevitably leads to sub-standard care because everyone is trying to go to the same person for a service and getting rushed in and rushed out. Most of us don't need the best doctor at X in the world to perform our services. It's like thinking you need James Gosling or John Carmack to write the code for your small business website.
By that logic, we should artificially cap everything. Why allow just anyone to be a programmer? Don't we only want the best programmers to write our software?
Any entrepreneur should be able to open up a licensed medical school. Anyone who graduates should be able to get certified as an MD. This is how markets should work - not capping doctors on the hope that we get "better" ones.
Also, I have seen some awful doctors, so I'm not sure the system is working.
Anyone who meets accreditation requirements can open a new medical school. The actual bottleneck in producing new physicians is downstream of medical schools in the residency system. Every year there are students who graduate with an MD degree but can't find a residency position.
I don't think we have to think of it as a binary opinion. The Association of American Medical Colleges (AAMC) realizes that the supply of doctors is an issue - but anyone can already start a medical school (California Northstate, for example).
And to address your point about "awful doctors", people are also starting to realize the shortcomings of the previous system - filtering too heavily on test scores/grades, for example, meant that many medical schools churned out graduates with great test scores but relatively poor interpersonal skills (which is a travesty since you're dealing with people all day) for a while. Nothing is changing overnight, of course, so the jury is still out in how things will be in the next few decades.
I would have much prefer having 30 minutes of time from an average doctor than 5 minutes of time from a great one.
Also we could quadruple the number of doctors we let in every year, and and we'd still only be letting in really smart hard working people.
And it's about choice, if you want to spend $400 to see the best of the best for 5 minutes go for it. But there are plenty of people who'd rather see a cheaper doctor for longer, even if there mcat scores weren't great or they got a B once in college.
Lastly a major chunk of what doctors do is pretty routine. Hey you have a soar throat, let's do a strep test, it's positive, here's an antibiotic. Or you say you have problems being happy, here take an ssri. Oh that one didn't work, let's try another one.
I suspect that is what is meant by "artificial", in "artificial cap". The idea is that we train fewer people than we could without a drop in quality (and further, make it difficult for already trained people from elsewhere to practice.
This is almost certainly true, and the incentives for physicians, medical schools, and banks are difficult to re-align.
Shouldn't anyone who passes through the training be considered qualified? If training is expensive then you no doubt want to prevent people from starting if you don't think they're likely to finish, but the metric there should obviously be a bar on absolute student quality, not rank. It should also be measured -- confidence intervals, correlation between input metrics and output performance etc.
I bet the marginal student in terms of acceptance is more than likely great doctor material, and I bet it doesn't drop off sharply right past them.
> Don't we want to make sure only the best and brightest end up being doctors?
No, you want people free to choose. If you want to go to the best and brightest, pay the best and brightest, and allow the others to get cost-effective care.
How would we measure that? How can we even measure that now in any kind of reliable way? Even you've been sick, or had a family member that's been sick, you know it's not easy. Plus, very few people can afford to pick and choose. I have no good answers.
No. You want people who are able to pass the STEP exams, complete an ACGME residency, and become Board Certified to end up becoming doctors. That is the only metric we should be using and, as it stands, there are significantly more people capable of overcoming those hurdles than the US currently allows the opportunity.
The reality is the "bar" ensures most people in medical and dental schools come from upper middle and upper class families.
It works to deter not those who are more than capable, but those that cannot incur huge costs to get into medical school. That includes volunteer time, extracurriculars, going on "mission trips" in undergrad to volunteer to help in medical clinics abroad, very expensive application costs (if you aren't in the 0.1% academically you NEED to apply to a lot of schools), paying to travel for medical school interviews, etc. Not to mention the opportunity costs of doing these things instead of working a paying job.
It doesn't end there. I have twice this year hosted friends from out-of-state that came to my city to interview for fellowships. Even after completing a residency most (all?) hospitals and medical groups will not pay for your travel to interview with them. One of these friends told me he is paying ~10k in travel costs to interview across the country for a fellowship position...thankfully he has a trust fund. I believe he faced similar costs when applying for residency.
It is insane. And that's just one aspect of medical education that deters otherwise great people.
If Cuba can figure out how to output a huge number of successful physicians (to the point that they placed them in other countries) there's no reason America can't other than apathy.
For the last few years, my medical care has been administered by a PA or a nurse...All the facilities around me are like that. 1 doctor for a few PA/nurses. I don't have major medical problems (that I know of...). But I'd rather have more medical professionals that studied for 8 years, than those who studied 2. If they aren't smart enough to be doctors, let the schooling weed them out.
I've had the same experience, but my complaint is that the services I'm going to them for don't require the services of a doctor at all. Most of the time, I am just going to get a prescription for something that I know I need, that for idiotic reasons I'm not allowed to just buy off the shelf.
Most of the time, I don't need Dr House. I need a warm body with a prescription pad. Occasionally a tailor, if I've sliced myself up.
That is a perfectly reasonable preference, but that the insurance system with unclear price differentiations makes difficult. You can make a copay larger for one and then people exert they preferences cost-effectively.
This actually would be my preference. I keep going to the same office because I have minor issues and the location is convenient for me. But one day I would prefer to see a doctor. Till that day, I should pay less for a "doctor's visit".
And actually, because I have a high deductible plan....I'm not paying a simple copay, but rather the full bill.
The other side of the story that's not covered here is that when hospitals buy up independent medical groups, patients, insurers and tax payers pay more.
In general, if a practice is hospital owned, they're allowed to bill about 2x what an independent provider could for the exact same procedure.
My wife is an ophthalmologist in private practice. A couple years back, we were looking at the economics of buying a laser to do a common treatment for patients with glaucoma, called a Selective Laser Trabeculoplasty (SLT).
Even with a decent understanding of medical reimbursement models in the United States, I was still kind of shocked by what I found.
The laser to perform the procedure costs about $30,000 to purchase.
The Medicare allowable for a physician performing the procedure in a standalone surgery center was about $315. There's really no reason that the procedure needs to be performed in a surgery center, and Medicare does let the physician bill about $30 more if they bought a laser for their office, and performed the procedure there. But, at an increase of $30/procedure, you'd have to be doing a ton of SLTs to make buying your own laser financially attractive vs. just using the local surgery center's.
Where things get crazy, is in terms of facility fees.
If a physician performs an SLT procedure at an ambulatory surgery center, the physician's Medicare allowable is about $315, and the surgery center can bill a separate facility fee of about $290, making the total procedure cost medicare just over $600.
If my wife's practice were bought by a hospital tomorrow, and they brought an SLT into her office, every time she performed an SLT in the exact same office that was now hospital owned, they'd be able to bill the $315 physician fee, plus a "hospital outpatient department" (HOPD) facility fee of $443, bringing the total cost of the procedure to over $750.
So, to recap the total costs to medicare:
Physician does the procedure in their privately owned medical practice: $345
Physician does the procedure in a surgery center: $600
Physician does the procedure in a hospital-owned medical practice: $750
This is why independent medical providers are getting bought up by hospitals and large health systems at an alarming rate.
You hear a lot in the healthcare market about the efficiencies of scale, and how large integrated healthcare organizations are doing amazing things. You don't hear a lot about the potential for independent practitioners to reduce costs, but it's absolutely there, and largely ignored.
I attended a talk by the president of a major academic hospital system. He talked about how his friends who were independent physicians would call him up and ask him to "save" them. Their practices were failing (probably bc the big academic center was so massive that it crowded out any smaller practices). The big system bought the small one, and overnight the previously independent practice doubled its billing rates. This was a core part of the strategy of the hospital system, as it is for hospital systems nationwide -- buy up small practices and use them as loss leaders to direct patient flow to the hospital profit centers (I've talked to people at these systems who view primary care as a loss leader even after their rates double when they are acquired). Then negotiate higher rates with payers since you control the market
There was no talk of benefits of better care coordination or data sharing through integration. Not in this talk or any of the other half dozen similar talks I've been to. "Population health" is a PR play that big hospital systems use to justify monopolistic behavior. And we wonder why healthcare costs are so high
You should expect EMR integration but I do know that it has not happened in many places where the local clinic carries the major group name but the EMRs are separate.. It's actually a shame. This is relevant to the Children's hospitals and clinics in Minnesota for example.
Trying hard to spin this as a reasonable effect, when the hospital buys a practice it also enforces all kinds of quality metrics that they need to maintain to get their insurance rates. Its true that a practice that changes no procedure will see a strange uptick in revenue, but those that update their practices, in principle, provide better care.
That aside, i believe this happens because it is illegal for a doctor to refern a patient and "Get a kickback". If the hospital really were the best place to perform a procedure, independent doctors have to be split between sending a patient out, which requires effort, staff & liabilities for the hospital to get all the revenue from it. If the doctor could negotiate with hospitals or other cares, they could do the work and get paid.
The justifications I've heard have nothing to do with the quality of care, and everything to do with subsidizing the costs hospitals bear for being required to treat uninsured populations who won't pay your bill.
E.g., if someone shows up at a private medical office and can't pay their bill, the office has no legal obligation to treat that person.
If someone shows up at a hospital emergency room and can't pay their bill, that hospital is required to provide emergency treatment regardless.
It seems like a horribly inefficient and inaccurate way to address this issue. I think broadly, the value-based model (where cardiologists are paid to keep their patients from needing expensive surgeries, instead of paid per expensive surgery) is probably the right model for the future of medical care, but I have doubts about how successful its implementation will be.
Interesting. Facility fees are being rejected by insurance companies or in the worst case passed along to the consumer which a lot of people are angry about. It might be worth writing to the CMS about or even the President. The Executive has expressed interest in more competition in the market. However, insurance companies should also be interested in paying a higher reimbursement rate minus the facility fee too since they'd have to pay that in the outpatient hospital scheme too (if they don't balk that is...)
Patients also (as the article mentions towards the end) get worse results, e.g., in [1] "Higher hospital competition was associated with lower 30-day mortality for three to five of the six study conditions, depending on the choice of competition measure, and this finding was robust to a variety of sensitivity analyses".
My local non-profit healthcare org was bought out by a giant conglomerate a couple years ago. They promised prices wouldn't increase. My monthly bill jumped 20%. It boggles my mind that state regulators approved this merger.
Both the prices and costs of a hospital/clinic are very much politics-driven.
And the most infuriating part to all of this is that whether a system does well financially has little to do with patient outcomes or any other metric related to human health. Yes, I understand Goodhart's law ("when a measure becomes a target, it ceases to be a good measure") since it's a common counterpoint used against my argument, but surely there are better metrics to optimize for other than profit?
For example, I work closely with a medium-sized reference laboratory, and it's clear to me that they have to take literally every shortcut possible in order to survive. The only reason that they're able compete in the market at all against a LabCorp or a Quest is due to the fact that they have deep political connections (lobbyists, governors, lawyers, etc) - certainly not because they have a better product or have better testing methods (although if you asked them, that's what they'd tell you).
>The only reason that they're able compete in the market at all against a LabCorp or a Quest is due to the fact that they have deep political connections (lobbyists, governors, lawyers, etc) - certainly not because they have a better product or have better testing methods (although if you asked them, that's what they'd tell you).
In my metropolitan area, almost all doctors are working for one of three very large and expanding private networks.
And more and more insurance offers are forcing members to pick a plan serviced by only one of those networks.
It may not be "government", but their healthcare is already dictated by a single large and not very transparent nor accountable organization. Where employees aren't worried just about making money, themselves, but also about maximizing "returns" for shareholders.
Indeed, it's hilarious that people are concerned about "socialized medicine" here when we already spend more public money on healthcare for worse benefits that any other developed country. We keep on passing up opportunities to do it right because our politics are so broken (to be clear: intentionally broken by one party who represents a minority of the population).
I saw something very interesting the other day. The Surgery Center of Oklahoma doesn't take insurance and they can't charge you if they make a mistake. Their post-op infection rate is 5% the rate of hospitals that get to bill your insurance for the infection you got. That is mind blowing.
It should be noted that you cannot bill Medicare or Medicaid for preventable infections that arise during a hospital stay.
I'll also say the statistical adjustment to actually make those infection rates comparable between hospitals is very non-trivial, and hospitals with low rates often tout them in ways I find fairly deceptive.
I think it is worth studying. In regulatory based hospitals there are natural profit incentives that are only gated by the law. The hospital has no incentive to go above and beyond the basic legal requirements for sanitation and won't if there is a profit based incentive not to.
Free market solutions where the consumer has strong rights usually leads to superior solutions and their result lines up with the hospital adopting free market methods.
"The basic legal requirements for sanitation and won't if there is a profit based incentive not to."
As I mentioned, there is not really just a 'basic legal requirement for sanitation'. There are significant financial penalties in the form of both uncompensated expenses and genuine cuts to reimbursement rates based on outcomes.
"Free market solutions where the consumer has strong rights usually leads to superior solutions and their result lines up with the hospital adopting free market methods."
This is not necessarily self-evident. For example, for many quality measures, despite their bad press, the VA outperforms private hospitals. Furthermore, many hospitals like the one mentioned in your original post are able to pick and choose their cases, which very frequently leads to lower rates.
I think it's worth studying as well, because it's my career. I am however also noting that you're making a couple false assumptions, and even measuring things like "Does Hospital A have more infections than Hospital B" are deceptively challenging if you actually want the correct answer.
Good points, and I'm no expert. I do think the VA outperforming private hospitals could be in line with it having different incentives, like fixed pricing and not being run as a profit mill. Different incentives due to a different non-free market structure could explain some of the other problems they have too.
This is just part of a general consolidation trend in the healthcare industry. Payers (insurers and claims administrators) have been merging to gain more negotiating leverage over providers and drive down prices. Providers responded by merging to maintain pricing power. The next step, which is happening now, is payers acquiring provider organizations to have everything under one roof. Essentially the industry is converging on the Kaiser Permanente model.
Well nothing much to imagine. It's true in most of the world that decent hospital treatment for serious ailment can bankrupt people. Now it is different in some rich european countries. But people here somehow behave as if apart from US one can get top notch hospital care anywhere in world without severe financial consequences.
I have seen here many who visit from US singing paeans for excellent healthcare in third world nation like India. It mainly works because 1) Whats very cheap for people in US is still very good amount of money there. 2) Local hospitals there would not dare ripping off Americans as it can cause great reputational harm if that incident ever covered by first world media.
However for locals these hospitals behave in absolutely atrocious and corrupt manner. And anyone not in top 5% in wealth pyramid will be ruined financially by treatment expenses.
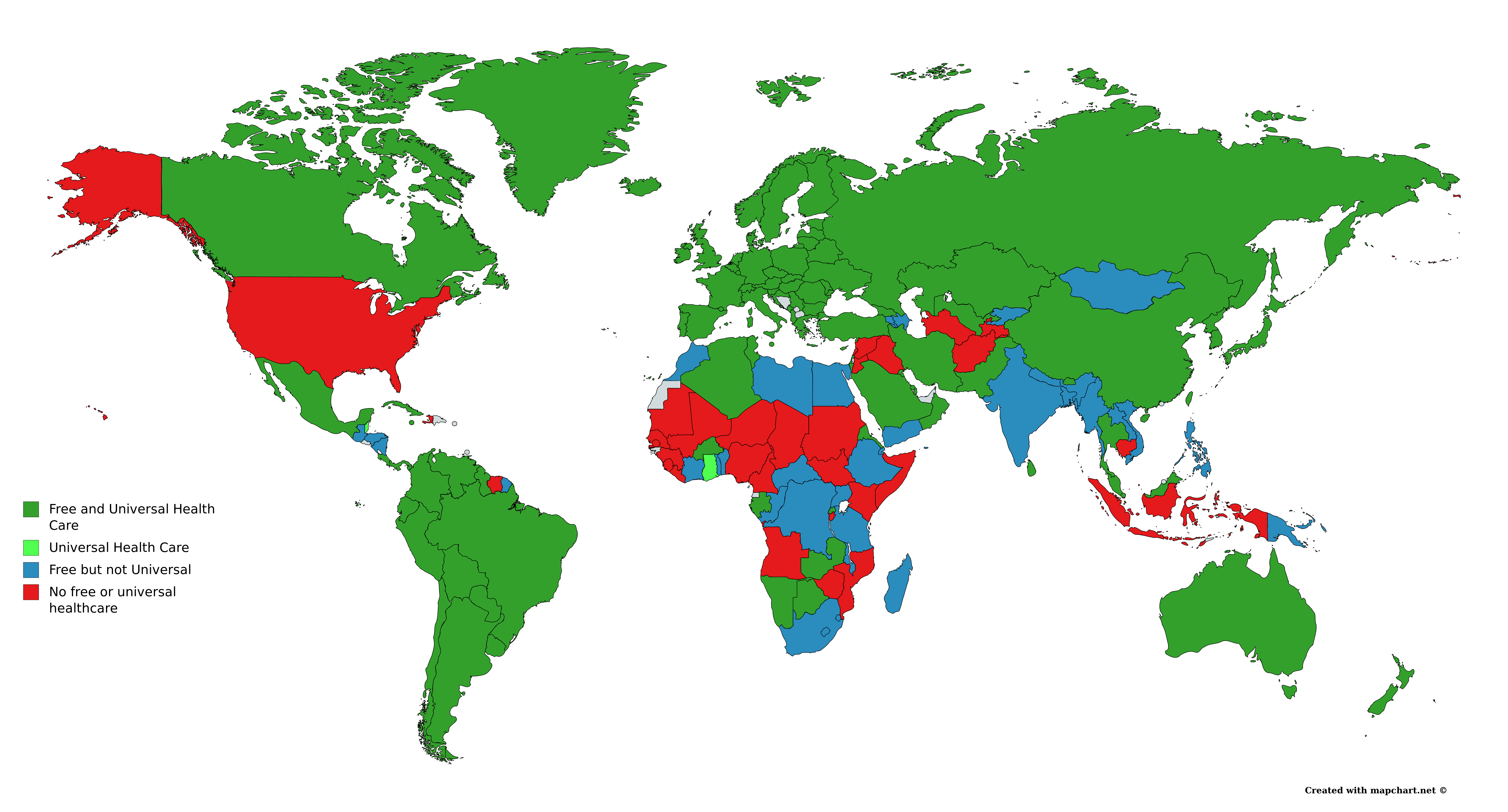
Meh, it's the norm in developed nations that medical care will not bankrupt you, period. You can fall off a cliff and break every bone in your body and in any of the green countries here, your out of pocket costs will be minimal:
It's not the norm in the undeveloped countries, which admittedly have a lot of population, but is that really the standard the USA wants to compare itself to?
Even in Saudi Arabia. The government might chop your hand off for stealing but even they take you to the hospital immediately and you won't go broke when you get the bill.
GP specifically said "decent" and gave an example of it being "present" but not "decent" for locals, and you countered with a picture only showing "present" which doesn't dispute what the parent said at all.
This comment seems sarcastic, but it’s literally what it feels like reading this and similar stories about the US medical system from another developed country...
It was indeed sarcastic, and in hindsight I apologise to anyone irritated by it. But yeah, it seems that a lot of US-based comments like to point out how terrible the alternative to paid healthcare is in places like India etc, but completely ignore the fact that comparable nations (i.e. Australia, Canada, etc) all have functional socialist-esque healthcare and it's kind of fantastic.
My personal opinion is that people are too selfish (I guess?) to even consider free healthcare as an option. At least, from the third person perspective, this is how it appears.
You might not be getting an accurate perspective of sentiment in the US. A lot of people in the US favor universal health care in some form or fashion. There are at least as many opinions on how to implement it, as there are countries with better systems.
But the opposition is strong too. Consider that if health care costs us twice as much as in other countries, it means someone is making twice as much, and they aren't going to give up that money without a fight.
People in the US have been indoctrinated by a lot of propaganda and not many see how things are outside the country. They just have never seen anything else.
I'm basically pro-universal healthcare at this point in some way, shape or form, but the one thing I don't understand is the role of private insurance companies in the aftermath.
They can't really just... disappear. People have jobs there, and stockholders own investments in these companies. You'd have to answer to a significant amount of people.
I feel like we've effectively enmeshed private interests so deeply into the US healthcare system that I don't know what it would look like without it.
>My personal opinion is that people are too selfish (I guess?) to even consider free healthcare as an option.
I believe that a significant amount of people in the US are too selfish to pay their taxes, let alone for universal healthcare, no matter what long-term figures you show them, so ¯\_(ツ)_/¯
For sure, private health insurers exist and in a big way. In Australia for instance, there's still privately owned hospitals which do offer a more "premium" level of service - i.e. better rooms, less surgical waiting times, ammenities, often where specialists have their offices, etc. Health insurance gives the option to use these hospitals and the insurer covers the majority of the costs. There's sometimes a 'gap' cost to pay.
The thing is, it's not like you might die in the public side of things and live in the private side - you'll get the same kind of primary care. But health insurance becomes a premium service for those who want it. I'm sure there's a lot more to the story as well, but it's one of those things that I'm not an especially full bottle on.
the tend to blame insurers for high medical costs (and hey it's easy not to like them), but the relative size of providers when negotiating prices with insurers is more likely
{kind=link}
1. "Rescue" the only small hospital in a rural area through merger or acquisition. The hospital entity is a "non-profit."
2. Over the course of the next year or two ramp up sales of the very much for-profit (and, conveniently, affiliated) health insurance plan, UPMC Health Plan to all major local employers.
3. Once sales of the health insurance plan reach "critical mass" within the community, the "non-profit" hospital becomes out of network, and ridiculously expensive, for all major insurers except one: UPMC Health Plan.
4. Within the year all local employers are basically forced to adopt UPMC Health Plan.
5. UPMC Hospital and UPMC Health Plan rates go up. UPMC Health Plan shareholders rake in the money while a small town goes broke trying to receive adequate healthcare.