I've spent a fair amount of time talking with nurses about the problems. I'm related to a bunch of people who are nurses across disciplines (ER, ICU, med/surg, etc). It's been enlightening hearing them talk about the problems...
1. Many new nurses make the same or more and long time nurses. It's frustrating when the nurse in charge with the most experience is making less than new nurses. Some hospitals are even trying to stop nurses from talking about pay.
2. Patients in COVID have become downright mean. Add this to the problems nurses have management and doctors (who are often rude and arrogant) and it's a poor culture. The quality of the environment, from a mental health standpoint, is on the decline.
3. IT systems that they have to use were designed by people who have not talked with the workers who use them. They may have been designed with laws and compliance in mind. Nurses aren't the people who choose or pay for these systems. But, they use them a lot (maybe the most) and it's obvious they weren't taken into account when designing the UX. It's maddening for them.
This one is big for product designers. Often we listen to the people who pay for it and miss out on the people who actually have to use it.
4. Nurses are the catch all for jobs. Not enough aides? Nurses do the work. Food service workers don't want to take food into a patients room... nurses will do it. Not only do they have higher ratios of patients but they fill in the work when other areas have shortages, too. So, the work per patient goes up. Pay doesn't go up, though.
The one I think you are missing is that nurses are and have been overworked for a WHILE now. (that's what I get from /r/nursing)
Hospitals have made sure they hire JUST ENOUGH nurses to cover shifts and no more. With covid hitting, this blew out the number of nurses needed resulting in a lot of "I know you've already worked 60 hours, but can you do another 20? we are short!".
Rather than hiring permanent people or upping salary, Hospitals have instead elected to just use travel nurses and an extreme premium so as to avoid any salary increases.
The fix is one that Hospital admins don't want. Pay your nurses more and hire more than the minimum to cover shifts so a nurse being out sick doesn't result in another working a 80 hour week.
So, instead it's been day old pizza with superhero stickers.
I actually think that this is just one example of many across a ton of disciplines where people like Nurses basically are forced to deal with costs and responsibilities offloaded onto them from above the responsibility chain. Resources are eaten up at the top of the chain to their benefit and costs are offloaded down the chain until it reaches people like Nurses at the end of the line who have to deal with it because there is nobody else to offload it to. There is no shortage of people wanting to be nurses (in some places it is extremely competitive), and there is a huge demand for nurses based on shortages everywhere, but somehow we are in a situation where nurses are overworked because they are short staffed.
I look at academia which is rife with money sloshing around, and see undergraduate classes are taught by grad students who make ~30k a year who are basically the Nurses of the academic world and treated like garbage. The justice system is dysfunctional, courts systems are overwhelmed and understaffed so criminals just enter and exit like a revolving door, and police is basically useless because the best they can do is taxi criminals into the system that automatically spits them out again, while they take the brunt of public criticism for how they are forced to deal with a problem that is mostly beyond their scope.
In all of these cases it seems like the bottom if falling out of these institutions, and the responsibilities have fallen on their respective janitors to deal with it when the solutions need to come from places that have been incentivized to create the mess in the first place.
"In any bureaucratic organization there will be two kinds of people:
First, there will be those who are devoted to the goals of the organization. Examples are dedicated classroom teachers in an educational bureaucracy, many of the engineers and launch technicians and scientists at NASA, even some agricultural scientists and advisors in the former Soviet Union collective farming administration.
Secondly, there will be those dedicated to the organization itself. Examples are many of the administrators in the education system, many professors of education, many teachers union officials, much of the NASA headquarters staff, etc.
The Iron Law states that in every case the second group will gain and keep control of the organization. It will write the rules, and control promotions within the organization."
Nurses, teachers, charity workers, IEPs, game devs.
These are all jobs where people sign up for the job. Whether it’s altruism or genuine passion. They’re willing to compromise and put up with less pay and harder working conditions.
But because they’re willing to compromise, these people are pushed to their limit. With not only low pay and shit conditions, but higher-ups which actively exploit their altruism and passion. “If you don’t work, patients / children are going to suffer!” coming from the same beaurocracy which created the situation where a) they suffer or b) you work extra hours.
They’re being pushed past the limit in fact, which is why there’s now a nursing and teaching shortage despite these actually being popular fields. A lot of people want to work these professions, they just don’t want the jobs.
I think most startups (at least originally) did start out as ‘change the world’. When you find out that changing the world is kinda hard, ‘become filthy rich’ starts to sound like a good alternative.
As a startup person, I like the startups where the spiel is “Get filthy rich by changing the world” the most. As long as I get to partake in the riches.
I've had good rapport with those who are honest about their startups being businesses, as they're usually also the same types who understand that working for them is just a job, and that a job at a startup comes with its own risks, as well.
People that go out of their way to say that their startups have a higher mission make me uneasy. I don't know if they're just trying to convince others that they're running something other than for-profit businesses driven by expected returns on investment for investors, or if they truly believe it themselves. It's either borderline manipulation or delusion, and neither are something I want to hitch myself to.
> Surely there's got to be some non-Musk company that I can add to that list?
Biotech startups? Develop a cure for horrible disease X (save lives, give people a few more years with their families, etc–feels good?)–and then get rich selling that cure.
I think Blue Origin's messaging is in principle similar to SpaceX (Bezos wants to save the environment by moving manufacturing to orbit, etc.) It is just that SpaceX rather obviously delivers on that message, and has grown rich delivering; Blue Origin hasn't delivered much yet, and it is hard to grow rich prior to delivery–but maybe, give them a few more years, they'll finally get their act together, and they'll become more SpaceX-like.
It seems to be the case that if you give someone a bunch of money, they'll stop wanting to change the world for the better. There are thousands of billionaires who could each end hunger and homelessness but have chosen not to.
The resources available to nation states dwarf those of billionaires, and it’s they’re specific actual job to do it, yet they too have failed to end hunger and homelessness. Bill Gates has sunk untold billions into humanitarian aid and its a drop in the ocean.
As a regular person, I like startups where the spiel is "Have a fabulous life and be pretty comfortable while doing things that even after some serious devil's advocacy seem as if they might make the world a better place".
I was impressed when I met the founders of Gaikai (a zero-day network game distribution system later bought by Sony), and asked them what the goal was. Answer: "Buy an island". Honesty has its merits.
I had a VP at a large company who was sharing her background. When she talked about her failed start up she said "we did it cause we wanted to be MILLIONAIRES... and that didn't work out so here I am".
It was funny and personable. Still one of the better VPs I remember.
It's one way to do it, not the only or simplest one? And once someone had done it, they tend to transition a bit to exploitation mode because why not (they think)? Is my impression
Yeah - the problem is that "a dream fuffilling job" without major filtering like med or law school effectively has a "virtual compensation" from desirability of the job. We see the reverse for (potentially literally) shit jobs or in ill repute. The economy accounts for your feelings but it cannot care about them.
They become nurses because it's a relatively easy (two years at a CC) to become an RN, and the pay is pretty good.
It's easy on the body, compared to similar paid blue collar jobs, like union construction. And it seems better than office work.
Durning the AIDS crisis a lot of nurses--who could quit did. They quit because many were legitmetly scared.
Hospitals got worried, and told their marketing departments to throw out the word, "We need nurses!". Most smaller hospitals had a hard time keeping qualified egos (The Medical Doctor), and they couldn't be bothered besides doing just the bare minimum.
Let's not forget their are many classifications of nurses (RN, LVN, etc., and porely trained Candy Stripers, or cheap help, hospitals (especially union controlled) use instead of nurses. Some are not porely trained though, but nursing unions don't like competition. I'm not berating unions. Moneynot spent on help seems to go to administrators anyway.)
(I went to school with nursing students. Most were divorced. Most were around mid 30's. This was in the 90's. Now nursing is a good path to middleclass for immigrants.)
"They become nurses because it's a relatively easy (two years at a CC) to become an RN, and the pay is pretty good."
That is no longer the case and many now require 4 year bachelor programs to be hired as RN nurses. My wife has her bachelors in nursing and runs an ER and the hiring requirements includes a bachelors degree in nursing and not a 2 year degree.
Leo Laporte would have him on a variety of his TWIT podcasts from time to time. I considered once coming up with a drinking game where you'd drink every time Jerry would have a sentence that included, "..when I wrote about...", but I realized you'd kill yourself.
That wasn't as apparent when he was a BYTE columnist for many years but boy his website sure turned into "old man yells at clouds" although he did have serious health issues in his later years.
As somebody with experience at NASA, this made me chortle. I would NOT characterize the average civil servant that I worked with as "devoted to the goals of the organization." That includes the lowest level field organizations. Unfortunately, for the average employee, it eventually gets treated like any other job.
It's possible this dichotomy works in theory only. Being generous, it's possible they just disagree about the goals of the organization.
That’s the point. The second group, those who only care about the existence of the organisation, and the power/money it provides to them, have taken over at NASA.
As a result only those who act to increase the power/wealth at the expense of all else, such as the original goals of the organisation, get promoted and hang around. The end result, an organisation that achieves very little, and consumes huge amounts of resources, full of people who really don’t care about the fundamental goals of the organisation.
Ok, I see your point and think you're right. The quote distinguished between scientists/technicians and management. I met many in the former group who cared little about the goals of the organization, but to your point, they had been within the organization a long time.
I don't think the technician/management dichomoty is a good proxy. There are people from both groups who care about the goals more than the organization, but they not the people being given power.
Anyone who has visited planet earth and spent time here is well aware of that. The task is to prevent these people from taking and holding power.
Note that the strict formulation of this law (ie. "in _every_ case..") is profoundly anti-democratic in that it assumes no democracy can ever exist or function. Of course, I hope your household provides a good counter example (if not, then you should seek outside support).
Anyway, for those of us who still believe in democracy, it has long been recognised that the cost of it is that everyone has to be a adult who takes responsibility for basic things in life like maintaining the social fabric of the institutions you belong to in order to prevent them from being taken over by sociopaths.
So the question is, will we support medical professionals in doing this? In the UK, before COVID, when junior doctors went on strike to try and remedy the situation, the media denounced them as enemies of the people and they were completely crushed by the state (with the help of their own professional organisations like the BMJ). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4902702/
>The task is to prevent these people from taking and holding power.
And for that I completely blame the 'right' thinking, honest, hardworking nerd types - even when given the reins to power they will often not take it, because it is uninteresting work, compared the cool gadget/problem they are working on.
> There is no shortage of people wanting to be nurses (in some places it is extremely competitive), and there is a huge demand for nurses based on shortages everywhere, but somehow we are in a situation where nurses are overworked because they are short staffed.
why is this such a common story across pretty much every single industry? There's more people in the country than 10, 20, 30 years ago. More customers, more money. Why do they think they can handle more work with less workers whose salary is less when adjusting for inflation?
Owners and operators have learned that they can keep the lights on by running their businesses with skeleton crews and, at the same time, reap the rewards of lower costs as profits.
Covid was also used to exploited the issue further and as an excuse for horrible service and skeleton crews.
During covid Business owners saw that the consumer was willing to take it so they will continue to run on skeleton crews as long as the consumer takes it.
Sure the consumer will complain but they are still using their money to buy from skeleton run places.Partly because most industries nowadays are Oligarch control and what one does the other does as well and the consumer has lost their control of the marketplace.
We are living in a world where the big guys have the majority control of the market place and the market want's skeleton crews.
This is seen across the board in all big business run industries. However with nursing, especially in the ER and the ICU that are now running a skeleton crew the consequence is your health and even your life. Until the big healthcare providers,insurance industry, hospitals, doctors , etc start to get sued over low staffing as the cause of death nothing will change and they know how to document to prevent such a case.
I don´t know much about nursing specifically but it is actually interesting to account for how many customers served per employee and how many there are at the bottom of the organization. If you are earning next to nothing and are doing 200 widgets per minute a 10 fold salary increase wouldn't change the cost of the product per customer. If there also is a large profit margin the desire to keep wages down is more of a fetish than the sensible choice it is at the other end of the spectrum.
Depending on the type of job you also get a different "product" depending on how much you pay and you might not be able to measure it. Employees cut corners in the least visible way and do not brag about extra effort if they are paid well enough.
This[0] was a fun read.
>Nursing care services are the most intensely used hospital services by acute hospital inpatients yet are poorly economically measured
[...]
>Nurses are an anomaly in the current inpatient billing system. Rather than bill for the actual services provided to the patient or the amount of time spent providing nursing care, the cost of nursing is embedded into the line item for room and board, which is the same fixed cost for every patient receiving the same level of care within a particular institution. In other words, all patients cared for on a given unit are billed the same room and board charge regardless of the actual amount of nursing care the patient utilized during that hospitalization.
> If you are earning next to nothing and are doing 200 widgets per minute a 10 fold salary increase wouldn't change the cost of the product per customer. If there also is a large profit margin the desire to keep wages down is more of a fetish than the sensible choice it is at the other end of the spectrum.
It depends on what portion of the cost of production is materials vs capital costs vs labor. You're presuming that labor is a small portion of the cost of production, which is probably true if you're selling them for $10. If it's an extremely low cost item, like plastic washers, labor can still be a significant part of the production costs. It also depends on whether you carry that down the supply chain, since part of your material cost is someone else's labor costs.
> Nursing care services are the most intensely used hospital services by acute hospital inpatients yet are poorly economically measured
This doesn't strike me as utterly insane. Most treatment prices should include the cost to have a nurse deliver it. The tiers of rooms should roughly approximate the amount of nursing care required outside of treatments. It's not perfect, but it might be better on the net than having nurses spend more time on the patient chart to add billing items.
I.e. it might be overall better to not have a specific line item for "rolled patient over to prevent sores" that the nurse has to enter in, and then billing has to argue with insurance about whether a roll was needed or not. It might be cheaper for everyone to figure out the average cost of providing nursing per tier, add a profit margin, and charge everyone that.
I'm not saying it is better, but it seems at least plausible.
> If there also is a large profit margin the desire to keep wages down is more of a fetish than the sensible choice it is at the other end of the spectrum.
I'm consistently surprised by misunderstandings of supply and demand.
There is a labor market. It's relatively free, all things considered. Sometimes companies conspire to keep prices down (see: high tech antitrust lawsuit/settlement) but usually the thing that keeps wages low isn't business owner collusion it's the availability of workers accepting work with a low wage.
Sure, all things being equal business owners would like to pay less for labor. They'd also like to pay less rent, less for insurance, lower taxes, etc. And sometimes they want to pay less than anyone is willing to accept, and sometimes instead of raising wages they rant about it on Twitter or in opinion pieces or whatever.
>usually the thing that keeps wages low isn't business owner collusion it's the availability of workers accepting work with a low wage.
But if you have a labor shortage and low wages at the same time, that means that workers accepting work with a low wage aren't available, but the employers are keeping wages low anyway. (And in this context, poor working conditions amount to "low wages" because they decrease the value of the job to the employee.)
In capitalism, "labor shortage" means "the employers had better pay their employees more, or else they won't have the employees to compete against other employers who will pay more".
I don't think we disagree, but what you describe is not necessarily a result of collusion -- maybe the business just doesn't work with higher-paid workers (i.e., product costs more than market is willing to pay) and scales with number of workers, in which case the owner might take whatever workers they can get at cost X, but can't hire any at cost X+1.
Only a profit-averse business owner would turn away revenue-exceeding-costs work merely because it involves paying workers more -- that business will likely not last super long unless there are special circumstances in play.
I think 'we have to exploit our workers to stay competitive' is a bigger argument against capitalism than 'I choose to exploit my workers because it gives me more profits'.
Because they really can in many cases from more automation, better tools, and better processes and understanding. The demand also doesn't neccessarily increase linearly with the population.
in many cases there is room for automation. I'm not quite confident we are at the level of an Auto-Doc assisting/replacing nurses yet, though. Nurses being thrown into multiple duties for 1.5x standard full time work seems to suggest that one or all of the above factors are not being met.
>The demand also doesn't neccessarily increase linearly with the population.
for elastic goods, no. But medicine is about as inelastic a product as you can get.
> academia which is rife with money sloshing around
In the academia that contains money sloshing around, the only grad students teaching are the ones who want to.
In the academia that doesn't contain money sloshing around, it's a different story.
But the truth is, no one in academia is making bank from academia directly -- not the grad students, certainly, but also not the adjuncts, or even the professors. You have to look higher up the chain (or, I guess, laterally?) for that. (Yes, there's the caveat that some faculty make good use of their prestigious affiliations or professional connections to increase income from outside of academia.)
I don't disagree nurses DESERVE to be paid more (I'm not sure if the economics bear out but they're certainly as WORTHY as many other professions), but wouldn't the fact that these nurses continue to work in nursing despite considering leaving bolster the argument even further that they are receiving adequate compensation?
Staying when you want to leave indicates there's enough compensation to 'make it worth it' at least versus whatever shitty alternatives you have. Leaving when you want to stay, to me, would be a much bigger indicator that nurses who want to stay in the profession can't because of wage/benefits/conditions issues.
> Staying when you want to leave indicates there's enough compensation to 'make it worth it' at least versus whatever shitty alternatives you have. Leaving when you want to stay, to me, would be a much bigger indicator that nurses who want to stay in the profession can't because of wage/benefits/conditions issues.
I think the conclusion of this sort of economic thinking is basically: Give your employees just enough money that they can keep they keep their head above the water but not enough to flourish, and just enough pressure/responsibility that they don't have energy to do anything else, but not too much that they have a complete mental breakdown that leaves them with the conclusion that they should leave your industry at any cost.
When you spent a lot of time and money into a specialized and demanding career, I imagine it practically very difficult to actually change your career, even if it's killing you. It's probably even worse if you have familial obligations. You likely do not have time or energy to better your situation after hours, and if you quit, you potentially resign yourself (perhaps) to many years of destitution while you accumulate the necessary knowledge to do something else. I would not be surprised if many people just bear bad conditions because the cost to do anything else worth one's time is simply too high.
It also cues your organization up for a failure cascade. You don't have workers who want to stay, you have workers who are forced to stay. As soon as they can leave, you're not going to lose "1 or 2" you're pretty likely to use a substantial plurality since whatever changed probably changed for all of them at the same time. Can your organization survive with 50% of the staff giving 4 weeks notice at the same time?
That conclusion would be fallacious, although many on both sides believe it. For one it ignores both growth potential and relative costs. High productivity workers can and do utterly dominate in ways which more than make up for it. And miserable employees are mercurial in quality at best relative to happy and motivated ones.
I recall hearing about one desert conflict "gratuitous" allocation of several times the prior typical water per day resulted in outsized military performance. I think it may have been the Six Day War. But Silicon Valley is basically the exemplar of that business model as they specifically go with a very high COL area in the world's richest country instead of mass outsourcing. Even assuming that the actor is a heartless and selfish bastard what truly matters first is net profit.
It is the same fallacious false economy seen both among slaveowners and the Soviet Union. That the labor is free or already paid for so don't worry about its efficiency.
The caring professions are quite a special case. The worse things get, the more carers care.
They are not like computer programmers who can make an industrial process be 10,000x faster. They cannot magically care 10,000x more, no matter how relaxed and comfortable they are.
Furthermore, as they are pushed closer and closer to failure, the collapse in patient care standards does not result in a collapse in profit. People aren't going to not seek medical treatment, it's a basic human need, sometimes a life or death need.
So we're back to the question: does that mean they should be exploited and milked of all their caring, at the same time the standard of care collapses, because the economic incentives reward that?
And that is fundamentally a moral/humanitarian question in which you have to make an adult moral judgement.
Employers are going to pay the minimum wages they can in order to retain sufficient workers. They obviously aren't going to voluntarily pay extra just so that employees can flourish.
There are a lot of jobs openings available to someone with an RN certificate and some experience. Unemployment in that group is close to zero. They don't all work in direct patient care roles.
It looks like you accidentally "did a communism" by arguing for nationalizing health and putting patient-care considerations above market considerations :)
Communism never has worked and never will work. We should just set legal minimum standards for patient care quality. Hospitals can then do whatever they need to comply with those standards, including setting nurse wages at whatever the market dictates.
Thanks Ayn Rand, a more astute reader might see the meme phrase, the scare quotes, the smiley, and see the obvious humorous intention :)
But I'll go ahead and explain the joke. There is a long history of the private sector using the spectre of communism (or socialism, or "big government" or "nanny state") as a canard to prevent sensible policies eg. anything that would improve patient care, even if it were at minuscule costs and will use that canard to justify lobbying aggressively to prevent it. And if they cannot obstruct legislative action then they switch to defunding the state bodies which enforce the regulations as an exercise in "cost cutting" because "the state is wasting your hard earned taxes!!" etc.
Hope you have a better rest of your day.
Edit: I mean, once you have set a regulation, and established a body to police it, you have already interfered with the market, so even what you are suggesting could be described as having "done a communism"
>Edit: I mean, once you have set a regulation, and established a body to police it, you have already interfered with the market, so even what you are suggesting could be described as having "done a communism"
Exactly, remove regulations from health care. I'm dead serious. Regulatory burden on nurses and health care workers are insane. It's completely plausible the net effect would be far more people saved than lost, due to greater access to healthcare and lower burdens to achieving outcomes.
Which specific regulations would you propose to remove? Everyone loves the idea of reducing regulatory burden but they always fail to give specifics.
For example, hospitals spend a lot of money complying with CMS reporting rules on iatrogenic harm such as bed sores and secondary infections. Should they stop doing that?
I love it. Libertarians and similar always like to say "communism sucks, can not work, can never work, is a completely broken model"... when the reality is that 1) they _dislike_ the model (which doesn't make it broken), and/or 2) that communism, like many systems, works well, until annoying corrupt humans wanting money, power or both start interfering with the ecosystem.
The second point is entirely accurate. It's one of the major factors that makes communism, socialism, untenable in many ways.
What's hilarious / frustrating is how these same people think that humans in a libertarian utopia won't be corrupt, won't want for money and power, and as a result, "Sure, remove all regulation - the market will get more efficient! It certainly won't end up like the railroads in the 19th century, or something out of an Upton Sinclair novel!"
I choose free markets BECAUSE everyone is corrupt, not the other way around. Regulators, who are third parties to the transaction beholden to neither those seeking health care nor those offering it, are the most susceptible to corruption. Regulators need eliminated to reduce corruption, amongst other things.
Never the supplier using ill gotten capital from predatory business practices to lobby or perpetrate regulatory capture.
Nope, it's always those pesky regulators sticking their hands out. Never those Captains of Industry! Paragons of Humanity and Unquestionable Beings of Moral Fiber and Impeccably Ethical Manner!
What part of that didn't you understand? Where did I say the captains of industry aren't corrupt. I said "everyone."
The consumer has the power to voluntarily spend or not spend with a particular health care provider for the vast majority of health care decisions. Their providers are beholden to the customer.
The regulator, on the other hand, is not beholden to the customer this way. The regulator, are typically integrated as part of government and thus not only are they unbeholden to the customer but they also are part of the same entity as men with guns who can use violence to achieve their ends. They are nearly always unelected and only in the loosest sense does the customer have any control -- no one seriously votes for their senators / representative based on who they approve of in say the FDA (can 99% of voters even name a single regulator in say the FDA?) -- that vote is dominated by other even more important issues you need your representative for. These regulators are effectively an ultimate source of corruption, backed by guns and only in the most tangential sense accountable to consumers but with wide latitude to control industry in ways that harm the consumer.
Yes everyone is corrupt, including the 'captains of industry' and even the 'consumer' but regulators make things massively worse. Regulators create an amplification effect of corruption.
Many can't afford to not work due to debt/rent/child support payments. If you don't pay rent you lose the apartment and the weekend parenting time. Miss the child support payments which were being taken from paycheck and child support enforcement takes driver license and starts process to take the car that is in your name.
That's actually my point. IF they are able to meet their obligations in nursing and their job is literally such a superior option to all the alternatives that they don't have 'optionality' then it's a weird flex to be angry at your one best(least bad) option that actually pays your rent and child support. Be angry that the alternatives aren't as good as the nursing gig you have.
I definitely feel for those paying child support, because 'imputed income' means you must pay at whatever rate the judge thinks you can make the best money at. You can never take a more relaxing lower paying job, because it will result in your imprisonment. Those people really have no future in the US -- their only option to throttle back their income is suicide, leave the country, or wait to go to jail. I blame society for the existence of these debtor's prisons, not nursing employers.
Seems you understand the more income -> more support trap. Mandatory overtime is considered in support calculations. That sets high water mark so going back to 40/hours week does not lower payments. I learned the hard way, and last employer I regularly sent email to boss thanking them for opportunity to work voluntary overtime. I would subpoena the boss's response of 'yes' for evidence in child support hearing to only use 40/hours week. The courts and county child support enforcement are wicked and liars.
Yes that never made the slightest sense to me. As someone married with a kid, when I get a raise or bonus it goes to my retirement -- not as a change in quality of life for a child who already has food/shelter/education. The kid still gets the same amount now as when I made significantly less. The idea that a kid needs more money because you worked overtime is quite possibly one of the dumbest ideas I've ever heard. At best it's simply backdoor alimony.
But the counter to that is, just because you work a minimum wage job and can't afford much child support, doesn't mean that what you can afford is enough to raise the child well. I expect it's very hard to say "the child needs _this_ much in order to be raised well" and then scale up from 0 to that amount as the parent makes more money. But you also can't just decide how much the child needs and then make the parent pay that much no matter how much they make. So the compromise is to base the amount paid on the amount the parent makes, and not really cap it. This has the benefit of allowing low earning parents to pay less, at the cost of high earning parents paying more (than is really needed).
>But you also can't just decide how much the child needs and then make the parent pay that much no matter how much they make.
This is basically how it works when you're married, though, at least in my family. Whether I'm unemployed or my work life is booming, the child cost the same for me as when I'm not. During bad times I liquidate my engineering tools / spend from savings / go into debt / sell my vehicle to take care of my kid if needed. On the flip side during the good times the extra money goes into investments and retirement. The amount I need to take care of the kid is fixed, with the amount I spend having virtually nothing to do with the amount I make. My level of personal real spending has changed very little since I got my first near minimum wage job after leaving home at 18; and definitely not linearly with my salary (at best I eat out more now, but that's because I'm busier making money). When the kid came they've always been a relatively fixed cost -- or at least unaffected by our salaries.
My kid would not be effected the slightest, better or worse, for my wage unless I was stuck below ~$12/hr for an extended time, so maybe it would make more sense to take a variable amount up to say $12/hr and then just a fixed price after that.
>doesn't mean that what you can afford is enough to raise the child well
Really depends. Some children grow up in situations where money is scarce but nonetheless have fulfilling childhoods that lead them towards success. It's also worth noting parents who can provide other things in lieu of money -- such as a homestead where they grow their own food and build their own house is perfectly acceptable in a marriage but somehow not acceptable as part of child support enforcement. It doesn't make sense.
>This has the benefit of allowing low earning parents to pay less
Again this is an odd choice. When I am making nothing, I still contribute half to the family costs. When I'm making 6 figures, my half stays the same. Both my wife and I have a deal where we pay half the costs. That way there is no resentment that someone is paying more just because they make more. It happens to be my wife makes significantly more money than me, but we still pay 50/50 costs of child and other bills with the remainder going into our own unshared accounts. It would be extraordinarily selfish and greedy of me for me to demand my wife to pay more simply because she makes more money, yet if we divorced this is precisely what the judge would order in many states. No matter how nasty the divorce I would simply return her share of her savings along with anything over half for spending of the child -- to not do so would make me a vile and greedy person who cowardly uses the violence of the state to unjustly take from others.
In our case the cost of the child is about 6-8% of our current salaries; so as you can see from child support calculators, about half of the money calculated by child support worksheets would be entirely for the lolz of the judge.
>So the compromise is to base the amount paid on the amount the parent makes
Unfortunately this isn't how it works, as above alluded. Once you make a certain amount it becomes your 'imputed income'. Once you set the precedent you can earn a maximum, the judge expects that to be your income you're capable of. You pay based on that higher amount whether you relax back to a lower paying job or not. In this way you're set up into a trap where if you try to get a higher paying job to save up to pay off years of child support, you're stuck in an even more fucked position and meanwhile if your kid is like mine and has a relatively fixed cost then the rest is bled off as backdoor alimony as a reward to your ex-spouse for divorcing you.
Well it depends what you think the purpose of economies is. One idea is that human beings are just a type of animal, and the economy is a social system which is supposed to incentivize the kind of behaviours that you want humans to do. If you want humans to be nurses, then the economy had better reward that.
Another interpretation is that the economy is a tool for exploiting people. For example, human beings are inherently of the opinion that human decency is good, they want to be functioning members of society, they care about the wellbeing of others, and if they are paid crap and treated like garbage, they will endure that, even to the point of great personal cost, emotional distress, mental illness, alcoholism, and even death. But as long as they don't quit, then everything is fine.
People don't 'switch careers' when they've spent years getting good at it. What they do instead is sit around posting on HackerNews and fucking the dog in all sorts of other ways.
Do you realize the irony of it all? This place gets like 1/10th the traffic on weekends. That's not a coincidence.
Are you familiar with the US? I don't see how you can in good faith argue that if people don't like what they have to do and/or what they get paid for it, they can just go do something else.
There's also the consideration that nurses don't leave, because they can see that patient care standards are not good, and they worry that if they leave, their colleagues will be forced take up the slack, employers won't replace them (since the colleagues took up the slack), and they will reward themselves for having found a way to "improve efficiency."
There are, of course, onlookers who are unable to even perceive the moral dimensions that normal human beings take for granted. Perhaps they were beamed down from the mothership just yesterday? The prevalence of psychopathy among human beings cannot be as high as it would appear from the average internet message-board, can it?
I am not really specifically making an argument on their salaries, I guess I am saying that Nurses are in the position where they have the least leverage in the system so they end up bearing a lot of the responsibilities that should be held elsewhere while having a disproportionate amount of resources allocated to them.
In healthcare I get the feeling that a lot of workers feel stuck in that there are many patients and people depending on them, and to leave would sort of be like abandoning them while increasing the burden on ex-cowoerkers.
> Staying when you want to leave indicates there's enough compensation to 'make it worth it' at least versus whatever shitty alternatives you have
Not necessarily. The "transaction costs" of switching careers are huge. If you want to make comparable money to nursing, you probably need training in something else, which likely requires a period of low or no income, possibly years of schooling or other training, etc.
It's hard to switch careers after 30 -- not always impossible, but certainly hard to revert back to the lifestyle of a 20-something for some time. People may stick it out despite unhappiness.
America is full of terrible jobs now. Just terrible. There has been a degradation of job quality with outsourcing, amazon, you name it. This may be why nurses don't leave.
But hasn't that always been the case, where 80% of the jobs were unsatisfactory in some way or another. Be it pay, conditions, co-workers, management/boss, hours, commute time, etc... Not just America, but most industrialized countries.
At what point in time did America have better jobs? A lot of people may reference the glory days of 70s and 80s manufacturing, but those jobs went from bad to good with the power of unionization. There was no free lunch.
This reads too much like a generalization of the standard complaints about management and their stupid meetings, the basic thesis of that web comic that was neither funny nor true, Dilbert.
The criminal justice system may be overwhelmed, but its reaction certainly isn't to just let criminals "exit like a revolving door". The US is still incarcerating people at 10x the rate of other wealthy countries.
Nurses being overworked is simply due to there not being enough nurses. It matters little if there's too much bureaucracy somewhere, or if too much money is spent on pharmaceuticals (about twice as expensive as anywhere else) or if doctors make too much money or if the US has a uniquely unhealthy population.
>Nurses being overworked is simply due to there not being enough nurses.
yes but this begs the obvious question of "why?", which either leads to the immediate thoughts of
1. not enough people want to be nurses
2. companies don't want to hire more nurses
I'm assuming #1 is false, so #2 is the go-to conclusion, at least on the high level. I'm sure I'm missing some more nuanced #3/4/5 explanations, but it does seem to ultimately come down to money that isn't being spent (be it maliciously or simply due to not having the budget).
The obvious #3 is "nurses are doing too much non-nurse stuff" which relates to both #1 (job is annoying and not what I want to do) and #2 in a way (they are not hiring non-nurses and/or investing in equipment, tools, etc).
I was introduced to the Dilbert comic strip while working in the Bay Area in the '90s. Customer's rep literally pulled me aside and asked how I could work for my boss. Said "this is your boss!"
Not just America but pretty much everywhere. I'm Finnish, and when I read about problems of American nurses it all seems pretty much identical to what is going on in my country, except maybe for some legal problems. Low pay, angry patients, lack of resources and bad IT seem universal.
The government is one of the few places where you can get a job in your twenties and retire comfortably in your 60s having made a decent, but certainly not outstanding, amount of money with consistent raises and cost of living adjustments.
What some people will call government waste - other people will call ethical employee treatment... sure there are a lot of other sources of inefficiency outside of your comment - but complaining about overpaid government bureaucrats is essentially advocating for the same race-to-the-bottom that has stagnated wages in large parts of the labour pool.
Please don't conflate State Public Employee retirement systems with State Teacher retirement systems. They each have their own rules.
The teacher retirement systems I know of have rules like (age + years_worked)>=80 ==> full pension benefits.
Retiring after 20y will earn you a smaller monthly and is only possible (under that rule-of-80 above) if you start teaching at age 40. Teachers are much more likely to retire after 25+y (age_start=30, age_retire=55).
A relative of mine works for a state level LEO targeting financial crimes - they've spoken often about how "smaller government" advocating politicians have repeatedly hamstrung the organization when it tries to go after large corporations. They've still managed to do good work going after smaller scale offenders that fleece investors - but I wouldn't put the blame on those employees for doing work you don't find useful... it's mostly up to politics.
That's the whole point. Powerful proponents of small government want to do anything and everything with no consequences. They've duped a lot of less-wealthy suckers into believing that having fewer public services will benefit them somehow, and/or that the only thing standing in the way of personal success is the government. They talk a lot about figures like word count in legislation and other easy to understand concepts (even to folks with low education).
Any govt office, focusing on the US here, seems to have a huge back log and understaffed like the IRS, Immigration services, DMV etc. For e.g. earliest appointment I can get is perhaps a month or two out. A huge backlog and understaffed makes a case of overworked employees. Surely, they are doing work, and so I can only think that by "they do too little useful work", you mean that the work itself that they do is of little use. Are they? Seems like getting my driver's license or tax refund is pretty useful, no?
It's actually not sure that they are doing work. There are backlogs because the employees and management are slow, inefficient, and don't make changes that would be made by a private organization either staying up to date or being replaced by a competitor.
(There are complexities and counter-examples that moderate this generally true statement.)
Defund the organisation to point of total chaos and near-collapse. Blame employees for collapse in work quality.
Here are some more generally true statements:
Increase profits and improve efficiency by cutting out maintenance tasks and firing the people who do them. Blame accidents or outages on employees, customers, bystanders.
People die? Company goes bust? Who cares? Even if there are consequences, the executives/officials to blame have already taken the money and moved on to the next thing. You can't prosecute them or get the money back (unless they were stupendously dumb and got directly involved and stayed on 'til the bitter end and centres of power were so affected that prosecutors can't ignore it: see Theranos, Enron, etc.).
Even without governments being overthrown, government agencies get deeply reorganized fairly often; often for reasons of politics rather than efficiency, but nevertheless.
We don't share preconceptions (I see multiple problems at multiple levels of public org charts, and in the electorate), but I see and appreciate why you might have that priority.
While I myself am frustrated with the bureaucracy and inefficiencies of govts, but I am not sure if its entirely fair to compare a govt with a private company/org - at least based on the scale they operate on and the profit motive, which make it very different.
> It's actually not sure that they are doing work.
> (There are complexities and counter-examples that moderate this generally true statement.)
Guess, based on that I cannot really have a counter argument here :)
From what I understand, queueing theory would say a backlog that doesn't go away but also doesn't keep growing means you're staffed to just barely keep up on average.
It's not given that the queue backlog is staying even, but you would also have to factor the externalities of better or worse performing offices into the queueing analysis. Slower government workers have consequences like the public giving up and bothering to add to the queue, and occasionally, lawsuits due to failure to perform a required task, legal cases being a less desirable budget spend than bureaucratic staffing.
Parents point is that there must be slack in a system in order to have a stable queue size.
But slack can also be perceived as waste, which can be cut.
And if your budget is cut, you are likely to see that slack as "first thing on the copping block" with the consequence that the queue begins to expand. But most systems have natural buffers which delay catastrophic failure. By that point there have been elections, you have retired, etc. and someone else is left holding the bag.
At that point you can blame the organisation for being "slow", or "inefficient", and then you can cut it's funding further, or destroy it outright or maybe outsource it to the private sector.
Then the private sector can drive profits by asset stripping and cutting safety or vital maintenance work, then when the whole system collapses, you can hold the taxpayer hostage by demanding a bailout of the, presumably vital, service (or you can renationalise it), and the whole cycle starts again.
Welcome to our planet, enjoy your stay, it's likely to be a brief one :)
Ah, if that was their only point, then I should have pointed out that a better operating department can achieve a lower waiting time with the same degree of slack. I understand the utilization rate tradeoff and that's not the issue.
I'm glad you've enjoyed writing your comments--like your style. :)
Ah sorry, slightly misinterpreted, my understanding was that without slack you cannot stabilize queue sizes which makes OP incorrect(?)
Yeah, more efficient nodes can delay that effect, but it seems that in real world system the existence of buffers means that consequences are delayed in ways that have significance (across careers, elections, etc) and those factors tend to dominate.
yw, nice that anyone reads it, without that i'd just be another mad shouty bloke on the internet, maybe i still am :)
I've worked public and private sector and know plenty of people in both and I've not noticed a huge difference in the number of people just coasting vs those who really try to make a difference.
What makes you think government is that much worse than the private sector in this regard?
> What makes you think government is that much worse than the private sector in this regard?
Sure a lot of people coast in the private sector, hiding in the corners of their organizations. But if the business allows too much of that to happen, they go bust. In government, they just go get a tax increase.
They do not go bust, they just find ways to bilk their employees, or customers, or the general public, or they find a way to make the government nanny them by shredding regulations or what not.
You seem to think that people cannot escape the consequences of their actions, and that consequences arrive swiftly and fairly. But I should think a quick look around the world we actually live in will disabuse you of that notion in short order. Especially when it comes to gigantic centres of power with vast reserves of cash and well protected revenue streams.
And if you've worked in any tech company, you've probably already seen that the people who coast do not "hide in corners" they make up an entire class, called "management", especially "middle management", they're front and centre because they have no productive work to do so they can devote the majority of their time to extravagant displays justifying their existence and their elevated positions and compensation.
One place I worked, was a Big Company providing overpriced services to other Big Companies. There were loads of low skilled IT workers, taking too long, making mistakes. Adding a BA and/or PM to drive every project when a competent dev could've done it solo a few years ago. But when you keep getting issues, you keep adding process and now every job is 1000+ hours.
But eventually the work got done and we kept getting work because Big Companies buy from other Big Companies. You're not going to risk tendering to a 3 man office who gets it done faster, cheaper, better because if it doesn't happen questions will be asked. Unfortunately there are a lot of talented small businesses out there but they just don't get the work due to this.
Do that enough, and Big Corp gets overtaken by a smaller, nimbler company that does better. See the book "The Innovators Dilemma" for one aspect of this.
Which Big Corp though? The provider or the consumer? The dilemma is, this all feels like a bit of a Boy's Club where they all agree to just help each other and ignore the little people. Not always formally, it's just how things work out. They have an interest in maintaining the status quo and ignoring upstart-startups.
Of course, eventually yes it's impossible to ignore the value gap. But I've seen companies threaten to leave but keep paying the bills for many years because in a big company, it's not really anyone's problem in particular and it's easier to just keep going along to get along. One example we had was B2C email communications, there are so many cheaper more capable players out there but they just got us to do it because we did other stuff for them.
> this all feels like a bit of a Boy's Club where they all agree to just help each other
Come on. They often try to sue each other out of business, get the government to declare competition illegal, "cut off their air supply", "knife their baby", etc.
> because we did other stuff for them
There you go. Not because of the goodness of their hearts.
Big Companies today are not the same Big Companies of yesterday. There is constant churn at the top. The ones at the top today are all newish companies.
Companies go bust all the time. One of the corporations I've worked for simply disappeared (Data I/O). Corporations disappear all the time. Remember RCA? No? How about Kmart? Sears? Kodak? Tektronix? Novell? Lotus? Wordstar? AOL? Zilog? Myspace? Zenith? Curtis-Mathis? RCA was once the biggest corp in the world.
I've known people in every corporation I've worked for who accomplished nothing and were not managers. I was often given the job of trying to turn whatever they did into something useful. Everybody knew who they were. I remember one person, we'll call "Smith". "Smith" would check in code, and it was always so bad that someone else would have to redo the whole thing. After a while, the term "smith-code" became a generic term for code that was worse than nothing.
How bad can you be that your name becomes a generic term for useless work?
"Smith" eventually got laid off. The team was relieved.
Sure, I was imprecise, I mean, they do not necessarily go bust. And even if they do, it can be delayed by decades, even centuries, by techniques that are too numerous and well known to list here.
I've known a few Smith's in my time, one thing they all had in common was the protection of a manager who had no interest in the quality of Smith's work, as long as Smith would take his side in any disputes. When the consequences became too great, the manager would suddenly understand the problem and approve the minimum of changes to fix it, while taking credit for the work. Smith would not complain about this slight because he understood the nature of the transaction.
Edit: btw. congrats getting rid of your Smith, these people can be very difficult to dislodge. Presumably your guy did not have the protection of a manager.
None of those companies have gone bust though. RCA got purchased and integrated by/into GE, Kodak filed bankruptcy but still exists with a significant number of employees, Tektronix is currently a fortune 500 company, Novell is now owned by Micro Focus, Lotus was never that big of a company, but they still exist and are doing pretty poor but still sell cars, AOL still exists and is owned by Yahoo, MySpace still exists and is owned by an advertising company and the other 2 or 3 I've never heard of.
The Lotus that the GP refers to is probably Lotus Development Corporation / Lotus Software, the makers of the hugely popular Lotus 1-2-3 spreadsheet from the 80s. It's still around-ish: it was owned by IBM until 2017 then was sold to the Indian company HCL Technologies for $1.8 billion. Pretty good for a company thought to be two decades obsolete!
Zilog was the maker of the Z80 microprocessor that powered a huge number of games consoles and simple computers in the 80s. Also still around - its parent company was acquired for $750 million.
I had to look up Curtis-Mathis because it wasn't a thing in the UK.
And MicroPro / WordStar International does seem to be legitimately dead: acquired by SoftKey who were acquired by Mattel who have since gotten rid of all the associated brands.
Yeah, I know they didn't literally go bust, some company always winds up buying the remaining value in the company, as its trademarks and IP have value.
But in any practical sense, they ceased to exist. (I meant Lotus of 1-2-3 fame, not car fame.)
You're right, I thought I'd remembered they'd gone bust.
> part of an umbrella corporation
meaning their former glory is gone. When I was starting out Tektronix was a very big deal in computers and electronics. I haven't even heard their name in 20-30 years.
The rules nurses have to deal with around things as asinine as taking PTO are AMAZING. They’re required to put in PTO requests months in advance and the hospital can and will say “Sorry, denied. We don’t have enough people…” As they are intentionally creating skeleton crews of nurses to wring every ounce of profit out of the business.
My mom was a nurse, my aunt was a nurse, my sister is a nurse and my best friend’s mom is a nurse. I really can’t believe anyone continues to be a nurse given the insane working conditions these folks have to put up with. Twelve hour shifts, overflowing with patients, watching newcomers earn more than seasoned veterans… When I compare it to my laid back software engineering job it’s like I’m living in an entirely different universe. The hospital industry is a hugely demoralizing place.
The hospital I work at requires physicians to file their schedules 8 months in advance. The only deviation from that is for emergencies. Unofficially there’s a lot of flex for them, but that’s the official administration line.
Yeah, my mom was a small town nurse it was the same even there. I gave them a bit more slack because it was a hospital serving like 2000 people (so not really a high profit place) but even there, there was a lot of last minute "Oh no! People didn't show up for their christmas shifts, could you come in please!"
In cases I'm familiar with, they aren't hiring JUST ENOUGH nurses, they are hiring AS FEW NURSES as they can get away with. More like half as many as they should. IIRC, nurse-to-patient ratio should be around 1:5, but it can often be more like 1:10 or worse.
On top of that, they also hire as few orderlies and nursing assistants as possible, so the nurse doesn't even have anyone to offload things to, and ends up having to do more work on more patients.
This has been a problem well before the pandemic.
It's a trope among nurses that they are so busy they don't have time to use the bathroom, let alone eat lunch.
Source: My wife is a nurse, most of her friends are nurses, and she left the profession ~a year before the pandemic because of exactly these issues.
This ended up being the last straw for one of my friends who was a nurse.
He kept getting vacation requests denied due to lack of staffing, yet if he asked if they were looking to hire, the answer was always No.
He was super lucky and had some early cryptocurrency investments pay off big, so he decided he was done with it retired. He said that he loved helping people as a nurse, but not at the cost of his own physical and mental health, having to work 60-80 hours/week. If he ever gets back into it, he would establish at the interview phase that he works 50 hours/week tops, and that vacation "requests" are not requests, but notices.
That describes me, though in tech. Trying to step back in to tech and recently had interview. After I explained parenting time schedule, HR guy said everbody works 60 hour weeks every week so there is not a role for me.
I believe there's studies showing that unlimited PTO policies actually result in people taking less time off, especially in competitive environments. The theory is people don't want to be viewed as "the guy" who takes more time off than anyone else. I'm not sure that's a good thing. There's less of that pressure when it's earned PTO.
This is so weird to me. I've always said I work 4 days, 32 hours, and that has almost never been a problem. I've once spoken to a prospective employer that really wanted 40 hours, and although the job sounded really interesting, 40 hours was not an option for me.
At all jobs, vacation time was almost never a problem. Maybe that's more the case now that I'm a freelancer, though. I just announce when I won't be available, and although we do try to plan things so that we never have the entire team gone at the same time (unless the company as a whole plans for that; Christmas breaks are often like that), they always accept my absense. It's really notifications, rather than requests.
But this is Netherland. We've got quite a different work culture than the US does.
That sounds perfectly fair actually. You explained you can't work 60 hours a week and he explained it's not the role for you. Complete honesty and the choice was made not to do the deal. You shouldn't get special hours or treatment for being a parent.
I agree with you, and I wanted them to know my needs so we all succeed. Hilariously the guy never asked my pay needs (low) and talked to me about the top of the pay range. I didn't care to correct him since the expectation was overtime all the time for everybody. Looks like a management culture I don't want to struggle against, so I can look elsewhere.
>The fix is one that Hospital admins don't want. Pay your nurses more and hire more
As someone who worked in hospitals to help redesign their processes, this one piqued my interest.
For every project I worked on (and I mean literally every one), the team lead wanted to jump to the solution that they just need the ability to hire more people. In the rare instances where they were able to convince hospital admins to do so, it never fixed the problem. Not once.
Why? Because it never addressed the root causes. They needed to take a process-oriented approach. There's a saying that adding more people to a broken process makes things worse. You can hide a lot of quality issues with inventory; if you have a requirements for 100 widgets a day and you have a crap process that only makes 10 quality widgets, you can meet your goal by increasing throughput 10x, but nobody thinks that would be a good approach. It's the same with injecting more staff onto a broken system. If the system causes nurses to spend disproportionate amounts of time on admin work and not on direct patient care, it may be better to look at your admin processes rather than just hire more nurses.
It's natural when people to feel overwhelmed to think the solution is to just hire more people, but it's almost always better to hold off on hiring until the system/process is fixed.
Edit: I'm curious about the downvoting. I think it would help illuminate the conversation if you could explain where your disagreement lies. I'm basing my statements on actually tracking when hiring was increased to the levels desired and metrics did not improve.
You're describing Brook's Law from The Mythical Man-Month. It was an observation of collaboration in software engineering specifically, and it cannot be applied universally to every industry. Really, anything that is highly parallel (medicine, teaching, stocking shelves, waitstaff, deliveries) can benefit from hiring more people until you reach saturation, and medicine isn't there or we wouldn't be having the conversation.
The problems are caused by a "just in time" approach to staffing, where you have exactly enough people to cover the shifts at bare minimum. What solution would you suggest other than more people? They are not saying to throw more nurses at patients simultaneously, they are saying to hire more nurses so existing ones aren't bound to spent the entire week stretching themselves across the hospital.
Also, I think you are being downvoted because you are applying software engineering rules to medicine.
It's interesting because they aren't software engineering rules. If anything, they are industrial engineering rules that pre-date software and certainly older than the mentioned book from 1975. The approach I was using was developed specifically for healthcare and with great effect in some organizations. I know this is HN, but I think it's an error to assume everyone is coming at a problem from a software perspective.
>What solution would you suggest other than more people?
It obviously depends on the situation but most of the time it comes down to reducing process waste. That may be automation through software where a nurse was hired specifically to only generate reports 40 hours a week, to re-designing a layout that minimizes travel time for nurses when they are delivering to patients. My experience with the staffing situation is that managers did not know how to staff to meet the needs of their patient loads and just revert to simple heuristics that left them understaffed at some times while being overstaffed at others.
> re-designing a layout that minimizes travel time for nurses when they are delivering to patients.
I think talking about micro-optimizations like this misses the forest through the trees.
It's neat and cool. Fun to wring out those last bits of efficiency. But the fact you even need to discuss it shows how hiring adequate amount of bedside staff is the absolute last thing any medical system will do.
> revert to simple heuristics that left them understaffed at some times while being overstaffed at others
Showing that they were better than modern day automated shift planning.
I will submit that if your hospital floor staff is not 50% idle on your average given fully-staffed boring day, you are understaffed. Only extremely exceptional events should cause your staff to be booked 100%. When it happens it should be root cause analyzed and be immediate cause for executive concern.
The trope of card playing nurses should be true, because of all industries there are - you want surge capacity in healthcare. Both physically speaking in terms of warm bodies available, as well as mentally speaking in brains not being stressed to their max the entire shift.
I understand these ideas don't end up with maximal efficiency. I am likely naive as well - but it's pretty clear that hospital systems are being operated in an intentional manner to keep staffing cut to the bone right up until the point the system or people break.
This doesn't just hold true for healthcare, it's endemic in a lot of service industries where the bottom tier employees are expected to live in service of the profession and take up all the slack from above.
There's a general rule of thumb that I have about any business: if it "looks busy" and people are running around, yelling into phones, unavailable for questions, etc., it's probably either understaffed or ineffectively organized. A workplace where things aren't visibly moving is one that is ready to make plans and respond to events smoothly. The productivity rate is somewhat independent of the "busyness rate" since there are a huge number of ways to stop work from needing to be done in the first place.
However, this seems to be unsatisfying to modern management styles. Apparently if you aren't running the employees into the ground like an Amazon warehouse, you're "leaving something on the table".
>I think talking about micro-optimizations like this misses the forest through the trees.
It may be different in practice than you are imagining. It's been years so I don't have the exact numbers, but something on the order of 10-20% increased patient throughput in radiology of a major metropolitan hospital that provides for an underserved community. (Keep in mind, it's not just nurses who have to traverse hospitals but patients. Many of them are old or lack mobility, so the changes are compounded.) I don't consider that "micro" but you may have different expectations. As a comparison, I don't think nurses would think a 20% increase in staffing is trivial, but my preference is to measure at the patient level, because that is the outcome I'm most concerned with.
>Showing that they were better than modern day automated shift planning.
Can you explain? I'm not following this statement. I was involved because it wasn't working.
>you want surge capacity in healthcare.
I agree. But like all complicated systems, you rarely get something for nothing. The trope in healthcare is you can choose between quality, cost, and access, but you only get to choose two. Lots of slack in the provider supply side is great for surge capacity, but it generally comes at the expense of cost. That's difficult when many of the same people who complain about the lack of providers also like to point out the cost of healthcare. I would prefer to take system-level view so we aren't essentially just shifting the waste around in the system and instead work to cut it out completely. In this case, excess capacity isn't waste but a desired measure of resilience. But I do think it needs to be measured and managed. My experience has been that nurse managers will just constantly increase the slack in the system rather than address the other issues.
And I absolutely agree there are issues, across many industries, where JIT thought-processes are short-sighted. COVID, and prior to that, Fukashima, has demonstrated this error. There are certain critical systems that we do not want operating at maximum input/output efficiency. If the staffing issues I've referenced were consciously framed in that sort of pragmatic, data-driven argument, I would be the first to stand behind it. But often they were really coming from a "we're-overwhelmed-and-don't-know-what-else-to-do-so-just-hire-more-people" perspective.
I'm suddenly reminded of traffic. For a long time, governments tried to fight traffic congestion by adding more lanes. Traffic is highly parallel, so this should work, right? But it doesn't. Traffic grows to fill up those additional lanes and you're stuck with the same congestion.
Here, better traffic design is necessary. And room alternative, more efficient forms of traffic (public transport, bikes).
I do think nursing (and many similar fields) do need to hire more people, but I also suspect they have to redesign how nurses work. Less overhead, more focus on the core of their work. Streamline the processes, especially the administrative side, and not expect them to fill in for many other kinds of work at the hospital. Get separate specialists for that.
> If the system causes nurses to spend disproportionate amounts of time on admin work and not on direct patient care, it may be better to look at your admin processes rather than just hire more nurses.
I get the impression that the same is often true for teachers, academics and cops: too much focus on administration, which takes the focus away from the reasons they chose these jobs in the first place. Streamline the administrative process, or have dedicated administrators help them with the boring stuff, so the nurses, teachers and cops can focus on the actual content of their jobs.
I would say streamlining is definitely preferential to do first and sometimes hiring staff afterwards. If the latter is done first it can quickly result in administrative bloat. I often wonder if that's part of the issue with higher education and contributes to some of the increased costs in recent decades.
If it's because it provides more patient care beyond what a nurse can provide in a good system, it might be a valid point. But if it's because the system is fundamentally broken, I'm skeptical that hiring more people will actually fix anything. From personal experience, it will only create a lag that will require the same need for more hires down the road.
I think maybe I'm miscommunicating the point. Yes, if overtime isn't needed people should be sent home. Hospitals agree on this; they don't want to pay overtime if it's not needed.
The issue I'm pointing to is that sometimes it's "needed" because of a bad process, like when there is redundant work. Sometimes it's needed because the system needs slack to compensate for disruptions in system dynamics. Sometimes it's "needed" because "that's how we've always done things." Point being, if it's needed, it should be because it contributes directly to better patient outcomes rather than bad processes.
And that seems to speak to his point exactly. The problem isn't that there isn't enough staff. It's the management is performing badly at scheduling or some other process. The internal problem needs to be fixed before hiring is increased.
The issue is that you hold this as axiom valid across industries. Since your personal experience with IT projects was that process was always issue, therefore when nurses say the hospitals need to hire more nurses, you assume they must be wrong. And you also completely ignore industry specific realities - like there being surge of patients due to covid.
Having excess capacity is necessary and should be a consideration to build a resilient system. It's not about trying to get to 100% efficiency, it's about managing to what you care about and resiliency can be one of those items.
It's hard to adequately staff to that level when the systems/processes are largely unmanaged. By definition, an unmanaged process doesn't know how much nursing gets spent on each element, from patient care to admin work. So it becomes just a guess as to how many you need; when people work in unmanaged processes they tend to feel overwhelmed and the knee-jerk reaction is to hire more people. And often when you add more people to an unmanaged process, the inefficiency can compound, leading you to feel like you need more people to fill the continuing gaps.
Hiring more people can be part of the solution. But you need to understand and manage the process first to get to the right answer.
How do you know the process is not managed? That is fascinating thing here - the argument is not that "I looked at nursing work in hospital and it was unmanaged" it is "I worked on IT project and since it was unmanaged, I am 100% convinced the same situation is in hospitals".
Maybe you meant to respond to someone else, but if you look through the chain of comments, they track back to a post where I was referencing personal experience in healthcare. This included projects redesigning processes where nurses were an integral part of the service.
My position is precisely that "I looked at nursing work in hospital and it was unmanaged." (not in every instance, of course, but certainly in those relevant to this conversation)
My Daughter was born on the winter solstice this year. We had a broken sink in our hospital room and someone came by to fix it. He had a trainee with him. Who was mentioning that he was scheduled to work New Years Eve and then again the next day on New years day. A 3rd shift followed by an immediate 1st shift. He was casually talking to the guy training him and mentioned that had to be a mistake. The guy in charge said something like "what did I tell you. They don't care about you". I sure felt angry for both of them at that moment.
The problem is not that they had to work on those days.
The problem is that they had two consecutive shifts.
The alternative is that the hospital hires enough people so they can schedule them such that everybody has time to go home relax and sleep after they are done with a shift.
My first year at the movie theater I had to work Christmas Eve, Day, New years eve and day, all for minimum wage. People are just more entitled now a days.
A good friend of mine couldn't get a single 3 day weekend approved (so one day of PTO) several months in advance.
Then I open my recruiter inbox and I see like 20 new B2C healthcare startups.
It really feels like the entire economy is designed to prevent problems being solved. Some people in healthcare are making massive amounts of money and the quality of life of everyone that performs the actual work has taken a nosedive when it was already a really crappy situation.
I think this gets it a bit backwards. There has been a shortage of nurses for decades, and it’s getting worse. This is exacerbated by an aging population and restrictive immigration policies. Travel/agency nurses were supposed to be load balancers for a system with variable demand for labor, but for a variety of structural reasons agencies began to pay nurses more. This has prompted a landslide of nurses moving into agency work. Labor costs have risen accordingly, but fundamentally that’s driven by the shortage of supply. If you talk to administrators they will tell you that they hate relying on agencies but they have no viable alternatives. They can’t raise wages because they have little/no control over their own cost structure thanks to the screwed up way healthcare in the US works, and most hospitals are barely scraping by. There are no easy answers to this one, and blaming it on shortsighted administrators (of which there are many!) misses the larger context.
>This is exacerbated by an aging population and restrictive immigration policies.
Sans the covid anomaly, immigration has never been higher in Western nations. The issue isn't restrictive migration. It's that we're not treating nurses well. That means fewer people pick this career, and more nurses leave prematurely. Suggesting that we need to import more nurses is only admitting that migrant nurses are willing to work for worse pay and worse working conditions, and I don't think that's fair to anyone.
> Rather than hiring permanent people or upping salary, Hospitals have instead elected to just use travel nurses and an extreme premium so as to avoid any salary increases.
In case people want an idea of what travel nurses made during COVID...
> In April, she packed her bags for a two-month contract in then-COVID hot spot New Jersey, as part of what she called a “mass exodus” of nurses leaving the suburban Denver hospital to become traveling nurses. Her new pay? About $5,200 a week, and with a contract that required adequate protective gear.
> Months later, the offerings — and the stakes — are even higher for nurses willing to move. In Sioux Falls, South Dakota, nurses can make more than $6,200 a week. A recent posting for a job in Fargo, North Dakota, offered more than $8,000 a week. Some can get as much as $10,000.
Travel nursing is definitely a great way to turn the tables if you can do it. The money you can make is clearly quite high! I fully support those nurses using travel nursing to get greater pay.
But it also isn't an option for everyone. Many don't have the flexibility to switch to travel nursing. For example, you may not be able to get a nearby contract and may not be able to travel (e.g. because you have children). Plus, traveling isn't an option for new nurses without experience, who now have to work in hospitals that are hemorrhaging experienced nurses to traveling AND have worse staffing ratios than ever.
These contracts are likely emergency contracts, which pay outrageously but often require a full week of 12-hour shifts or something similar with the expectation the nurse will only do one week then recover. I've seen this for COVID peaks and when a hospital's entire nursing staff is planning to strike. The $5200/wk rate is more likely 3 or 4 12-hour shifts.
> The $5200/wk rate is more likely 3 or 4 12-hour shifts
3 or 4 12 hour shifts a week is normal for salaried nurses. $5200/wk isn't. It's over double.
> which pay outrageously but often require a full week of 12-hour shifts or something similar with the expectation the nurse will only do one week then recover.
I'm not sure what you're trying to say. Yes, it may be a full week of 12 hour shifts, but it's still a much higher pay. And if you get the next week off, it's a fantastic deal.
For context, pre-pandemic, I knew a nurse who often would do this schedule for her salaried job - she requested it as she liked having a full week off.
What I mentioned elsewhere: Travel nurses have a lot more control over the contracts they take. They can work fewer hours per year and still make significantly more. They may have stretches of long hours in a given contract, but annually they work less.
> 3 or 4 12 hour shifts a week is normal for salaried nurses. $5200/wk isn't. It's over double.
It's a normal shift schedule, and they pay travel nurses much more than staff nurses to work the same shift schedule. These are typically 3 month contracts, but not always.
> I'm not sure what you're trying to say. Yes, it may be a full week of 12 hour shifts, but it's still a much higher pay. And if you get the next week off, it's a fantastic deal.
I don't disagree, but a lot of people do not want to work (or feel like they can't provide good care for) 12 hours every day for a week.
I haven't found concrete figures, but from what I've read, they do often work more hours during the contract. However, travel nurses in general have far more control over their schedule than regular salaried nurses. A salaried nurse cannot refuse to work, but travel nurses routinely say "No" to contracts if they don't like the pay or the hours.
What happens is they'll accept a few weeks (or 2 months) of long hours, and then take a month off and relax. As you can imagine, if they're getting paid $6000/week, they can easily take a lot of time off and still get paid more annually than their salaried counterparts (while overall working fewer hours per year).
I replied to the parent, but the highest quotes are probably emergency contracts for 5 or 7 shifts of 12 hours but only for a week. Longer contracts are often 3 months at 3 or 4 shifts per week.
Executive hospital pay is ridiculous AND the executives are often times just some MBA type without any real value add. How about you chop up their comp between the nurses - would be a start. Nurses are the lifeblood of the hospitals for anyone who has had the unfortunate circumstances of having to spend any time there.
>Executive hospital pay is ridiculous AND the executives are often times just some MBA type without any real value add.
I can agree that executive compensation is exorbitant, but do not agree that "MBA types" (what does that even mean?) have no value add. There's nothing inherent with being in the health care industry that translates directly into administering a (large) business. Why would you think doctors or nurses would be good at that?
The administrative side typically doesn't actually understand the technicality of administrating care and many times are MBA business types who administer a business as if its is commodity without understanding the true nature of the business (from their overconfidence generated from their degree and their lack of understanding the nature of the problems through distillation and non-technical understanding). This MBA culture is similar to tech/prod relationship in tech companies. Thus they provide little value add and get paid unfair amounts for their relative value.
I agree that Doctors and Nurses would likely be poor administrators - however the disparity in income is incomprehensible in healthcare.
I would add that travel nurses are treated better in a lot of ways. Staff nurses must attend certain meetings and training aimed at standardizing care and improving outcomes. The travelers don't have to attend. Travelers can take off pretty much any time they want as long as they know before they sign the contract. Sure, they're considered "outsiders" by some staff and sometimes get the less enticing patient assignments, but for those drawbacks, they get paid 4x (I've seen 3-8x staff rates, but 4x seems common) plus a housing stipend as long as their location is more than some distance (I think 40 miles iirc) from their "home" location. Why would anyone be a staff nurse?
Anecdotally, I know a travel nurse who works in pediatric ICUs (PICUs). One shift a couple months ago, the overnight staff on her unit was >80% travelers. And this is in peds units that aren't as affected by COVID, because ~1/2 of the patients are cardiac babies with congenital heart issues. The only case I can see for not paying staff more to increase retention is that they can respond to a dip in cases over the summer, but that can't possibly be an 80% decrease in patients. Maybe they're waiting until travel rates come down to offer an increase in pay so their 1.2x salary offer is more enticing in comparison to the travel rates, but the current system is ridiculous financially. I did mention that we've seen first-hand that hospitals can afford to pay nurses $4k/week, though, and I'm sure I'm not the only one who noticed.
> Hospitals have made sure they hire JUST ENOUGH nurses to cover shifts and no more.
This is a two-edged sword. If you hire more than you need, the nurses' hours will be cut during normal situations and they won't make enough money. If hospitals don't cut extra hours and instead keep the staff on the clock, a public scandal will erupt surrounding well-paid medical professionals sitting around doing nothing.
> a public scandal will erupt surrounding well-paid medical professionals sitting around doing nothing
I don't think that's true. Increasing the amount of nurses means simply increasing the amount of care. If you have twice as many nurses, you'll have twice as much care for your patients. No way nurses would be sitting around doing nothing.
Not sure why you're being downvoted, but the idea that doubling nurses doubles the amount of patient care shows an ignorance of the healthcare system. "Patient care" is a nebulous term and needs to be further defined in that statement. Do you now get two catheters instead of one? Or get your vitals taken twice as often? Both double patient care but only one is relevant.
I could definitely imagine nurses having twice as much time to carefully read my charts, or twice as much time to sleep at night and be well rested so they don't fuck things up, or being able to come by and help with something twice as quickly
That would provide better patient outcomes, I agree. Whether hiring more nurses translates to actually doubling that, is another question. To be clear, I'm not saying that increased staff is not part of the solution; it's just been my experience that it's rarely the sole part (or often even the majority part) of the solution.
It's because it would actually double the amount of care on most floors, because they're usually at 60% of the staffing they need as a start because they've been able to get away with that for years.
That doesn't really answer the question. "it would actually double the amount of care". It would double the amount of staff hours. How those staff hours are used is a measure of patient care and not all hours are equally relevant to the patient.
As an example, if we assume you are a software engineer and you double your work hours, will you double your code output? Probably not, just like it's not a 1:1 translation of nurse hours to patient care.
Comments like this are showing just how much you don't understand maintaining a service level based care, and are stuck in thinking in terms of producing a product.
Combined with willfully ignoring that basically all floors are intentionally understaffed and have been for years.
I can tell you from my years in healthcare that many of the people who think they know how the system works only have a very myopic understanding and they usually are the one's who have the most confidence that their simple solution will fix the problem. Unfortunately, there's a lot of nuance in complex systems like healthcare.
We probably agree about the staffing levels to an extent, but I would be curious to hear the staffing estimation methodologies used in your experience.
I wasn't healthcare admin and most of my department was staffed with nurses. But we were very data oriented and it helped buffer us from emotional responses to problems.
I have no doubt your emotionally detached analysis decided the floors were adequately/overstaffed since the nurses hadn't all quit yet or gone on strike.
I mean they clearly are still working there, they can always do a bit more to cover right?
I think you are are either misinterpreting my stance or transferring an argument from your personally experience. Also, you may want to revisit the HN guidelines[1]
My position is not that they were always adequately staffed, but that in my experience increasing staffing did not fix the problems as expected because the problems were rooted in more systemic issues. As I've stated elsewhere staffing may be part of the solution but rarely a panacea. Also, my stance is that fixing the systemic issues will help them do less non-patient-centered work so they can focus more on being a healthcare provider, where they are the most valuable.
At the rate that healthcare charges in the US, hospitals can more than afford to keep X+1 or +2 needed nurses around in three 8-hour shifts. They just don't.
Not even close. Most hospitals have trouble staying afloat as is. And there are disciplines within nursing, so you'd have to overstaff by quite a bit more such that closer to 2x is a backup but leads back to the GP's point.
They employ on-call, PRN, contract nurses, etc to fill in the gaps which mostly works in non-pandemic situations.
Reading threads like this really hammers home most of HN have never worked in health care. Hospitals BARELY make their budget. 1% over cost of doing business is considered a really good year for my institution.
Also if I never have to hear people complain about bloated admin budgets in education and healthcare ever again it’ll be too soon. Those admins aren’t sitting around on their thumbs—they’re dealing with the ridiculous legal and administrative system the insurance companies and government have created. Those people are absolutely critical for the institution to exist.
This seems to be highly bifurcated, like so much in the US, between the haves and the have-nots. But overall I don't think it's fair to say "Hospitals BARELY make their budget." As usual, the whole system is broken. There are some hospitals with a wealthy customer base with full-ride insurance who can bill obscene amounts and profit massively, and then there are some hospital systems with uninsured and underinsured customer bases who are just scraping by.
I looked up my local hospital network, UCHealth (Colorado, there are many UCHealths it would seem), and their EBITDA in 2021 was 16.6%. Mayo Clinic posted 1.2 billion dollars in _operating profit_ in 2021, and also have a gigantic investing arm with several billion dollars under management.
Then we look at networks like Spectrum in Michigan, who posted only a 3.6% margin, or Henry Ford, with a negative operating margin offset by investment income, and it becomes clear that _some_ hospitals barely make their budget while _others_ rake in dollars.
It’s the same economics that create food deserts in some places and Whole Foods in others. Or how banks don’t exist in poorer neighborhoods despite being profitable on others. There is no incentive to allow one to subsidize the other. It happens with health networks that are mission based but otherwise, not usually. Try balancing out your research with the taxpayer funded public hospitals, it’s a train wreck.
Non-profits generally use substantial income in excess of revenues for expansion, just like many for-profit organizations. Excess revenues can also be absorbed in salary and other compensation or cost increases, usually top down of course. The main difference is that non-profit organizations are prohibited by law from making distributions to owner-shareholders. They can spend excess revenues in any number of other ways, starting with the furniture for example.
How badly is the entire industry mismanaged if hospitals have to charge thousands-to-millions of dolllars for treatments? There is no possible way that is just barely supporting facilities+medical staff+reasonable administration+liabilities if other countries can do it at tiny fractions of our price.
Instead, the story as I've heard it seems to be similar to education: massive administrative overhead permitted by fundamentally broken insurance billing.
Sure I may not know healthcare but they really need to fix their shit.
I agree it needs a reboot but it’s highly politicized and the things they reform usual cause more and more administrative burdens and thus costs.
The sad truth is labor in America is incredibly expensive. Healthcare is extremely labor intensive. And everything else is expensive too. We don’t pay the came cost from the source for things like drugs, medical supplies, etc. A thing that cost $100 in another country costs $1000 in the US. That’s from the manufacturer who can control what price they charge. It’s capitalism doing it’s thing. But we also have a ton of middle men. Insurance, brokers, wholesalers, distributors, and on and on. All of who need a margin of profit and maintains some level of administration overhead. So when people here say administrators and too bloated and over paid, it’s really the supply chain that is deep and prices that are uncontrolled.
Even parts of this thread exemplifies how difficult it is to get agreement on what the problem/solution even is. People are complaining that healthcare is too expensive others saying nurses need to be paid more or have hospitals increase staffing. These ideas are in complete opposition.
I’ve never seen that even before the pandemic. 1.5x-2x is normal for all the usual reasons a contractor cost more. Taxes, benefits, agency that needs a margin, etc.
I’m guessing if you’ve seen that is hyper localized to some place/issue.
1.5x isn't a real increase in staff rates if all it accounts for is taxes and benefits that the employer covers for regular employees anyway. It is like certain government employees who complain about being paid too little when the actual cost of their compensation in many cases is through the roof.
The situation is so bad that regulation or standard practices encouraging employers to document compensation figures instead of quasi-mythical salary figures would do a lot of good to reduce confusion in this area.
All in, it's still averages about 20-30% more expensive in a normal operating environment (before pandemic and all the subsequent issues). This is significant on the largest expense line item and considering it's controllable to a degree.
You can pay people fixed monthly salary + overtime hours. You don’t need to cut their hours and their pay, though that’s often the choice that employers make.
Exactly, choosing to cut hours or pay due to a lull in business is a choice made by the employer. It's not like these hospitals are sputtering along right at the fringe of solvency and one bad choice will bankrupt them - private health providers tend to make pretty comfortable profit margins and the fact that they can pay such outrageous surge prices for travel nurses is a pretty clear proof of how much they have to spare.
Many hospitals literally are sputtering along right at the fringe of solvency. This is particularly a problem with non-profit hospitals in poor and rural areas. Summer have shut down in recent years, and the pandemic is accelerating that trend.
Some hospitals are sputtering right along, and a list of 12 isn't a great piece of evidence that those hospitals (many of which are run by regional organizations which are essentially consolidating patient pools into a central location) are being run effectively - especially if these hospitals are paying 10k/week for travel nurses.
If there's a location that isn't profitable to operate a hospital in then the hospital will probably fail. America is the country still clinging to market-driven healthcare services and the market can be a cruel mistress.
And all that doesn't at all erode the fact that nurses are paid pauper's wages at extremely profitable hospitals - some tech companies are going out of business, some probably closed their doors today... that doesn't mean that all engineers are expected to work for 60hrs/week at $15/hr.
That article was just a recent example. If you search around you can find many other hospitals which have closed down or gone through bankruptcy in recent years.
> Rather than hiring permanent people or upping salary, Hospitals have instead elected to just use travel nurses and an extreme premium so as to avoid any salary increases.
Hearsay from the nurses I know: a large hospital near me has a separate budget line item for full time nurses vs. travel nurses or other "mercenery" roles. This incentive system will never create the best patient care, but I suppose that's not really the goal.
for those that aren't aware, a while here reads as at least 40 years, and it gets worse every year, especially the last 10 or so.
With additional nuance that this kind of thing used to be protected a bit by the additional guard of a pharmacist. The automated dispensary changed those criminally liable people into a checkbox bypass that this nurse (and from the sounds of it, the rest of them by effect of policy) regularly bypassed.
I always wanted to understand how hospitals get away with treating their employees like that. In any other industry, people would not accept it. This is the industry where (arguably) I'd want people to be _most_ relaxed and _least_ overworked because human lives and wellbeing is on the line. Why don't airlines do that to their pilots? Should there be similar regulation in nursing?
Same reason game developers get treated like shit compared to many other developers. People are willing to put up with more shit to do a job they find rewarding.
Not at all. I'm saying people consider all aspects of a job when choosing whether to leave which includes pay, working conditions, personal satisfaction from doing the job... Healthcare people probably like the feeling of helping people in need and are willing to accept the tradeoff of worse working conditions over choosing another job which does not have as much personal satisfaction of helping people but better working conditions.
Game developers are likely the people who love video games and so are willing to put up with the worse working conditions in order to work on the games they love.
and now nurses are apparently solely responsible for medical errors and will not be supported by their employer. the cause of which appears to be related to #3 in GP above where overrides are a regular occurrence and quickly loose meaning if you have to do it multiple times per day.
I always thought it was insane how nurses, a health profession, are forced into so many unhealthy habits, like working long hours with little sleep and with difficult access to healthy meals while they are working.
On an individual basis, nurses are overworked because they choose to be and their employers allow for it. The standard work week is 3 12 hour shifts, which is much less than most professionals work. Like a retail or warehouse worker, they are expected to clock out as soon as possible and leave when the shift ends. Those of us with salary jobs knows how difficult that can be in our arrangements and how much "free" work we end up performing. They get paid premiums for everything; night, weekend, etc. And since they're hourly, they typically LIKE the overtime and signup for it as much as possible. They also might work FT at one hospital and pull extra shifts at another hospital on a PRN basis. These things are very common. Just like in a retail environment, people typically LIKE to work holidays so long as it's voluntary because it's 1.5x pay (or more?).
> Rather than hiring permanent people or upping salary, Hospitals have instead elected to just use travel nurses and an extreme premium so as to avoid any salary increases.
This makes no sense. Capacity is the problem, paying more for the same capacity does not solve the problem. Hospitals try very hard to avoid overtime and the travel nurses due to the cost. It's also a very elastic model to balance and a lot of flex (non Full Time) folks are needed to fill the gaps and manage cost somewhat.
> The fix is one that Hospital admins don't want. Pay your nurses more and hire more than the minimum to cover shifts so a nurse being out sick doesn't result in another working a 80 hour week.
That is the current system. The problem is usually time. If someone calls in sick, they do it an hour before their shift starts. They usually can solve for this. Either they call from their roster or a supervisor level person with an active RN license steps into the clinical side that day. Staffing at 2x just in case everyone calls in makes no sense. Staffing at 5x just in case a pandemic hits makes no sense.
Hospitals barely make money as it is, I don't see how this is a sustainable solution. Paying more does not create capacity in this industry.
It's also important to note that "nurse" is a very generic term. For example, ICU nurses is a very distinct type of nurse that has been dealing with COVID first hand (caring for vent patients). They are the ones you hear about making $150-200/hour in COVID times. It is difficult to become an ICU nurse. It hasn't been possible for a surgical nurse to pivot to ICU nurse in these times so the labor pool has been rather fixed, or shrinking due to natural churn and inability to onboard new folks. It would be akin to suggesting why does some [insert super specific domain expertise] developer make $1M/year at FAANG when they could hire a PHP coder for $15/hour on a freelance website. There is no immediate/cheap substitute for the experience and knowledge that the expensive developer has, so they cost more. This is happening in nursing where some are thriving while many actually got furloughed early on in the pandemic.
My personal opinion on the matter, is one only has to look at the demographics of an average nurse. It's become quite "old" and like other industries, the boomer's retiring is causing a labor issue. The handful of nurses that made 5-10 years of salary since Q1.2020 are now ready to retire early as well. I don't blame them.
"Hospitals barely make money as it is, I don't see how this is a sustainable solution. Paying more does not create capacity in this industry."
The problem is – and this may be very bizarre in a society as capitalistic as the US – healthcare should not be beholden to making a profit.
Rehabilitating people is clearly "valuable" to the economy in that without people to participate in the economic system, a debt-based economy collapses; I'd argue that healthcare is much more valuable to capitalism than is reflected on a balance sheet of paper costs/revenues/profits, and yet a system such as ours has absolutely no way in its current form to price that in (sure, in an academic defense you could wave hands that "positive externalities" such as these should be priced in to the model, but it's clear with the racket the medical industry has found itself in that will never happen practically).
The main issue profit-seeking conflicts with is that whole rehabilitating/healing/saving people is an intrinsically good thing to do, and that letting people who have full lives to live die or suffer is an intrinsically bad thing to do.
What's not sustainable is that healthcare has to survive within the confines of a system that is many times in complete opposition to it. Other otherwise-capitalist countries have at least tried to insulate their healthcare industry from market forces, meanwhile the US has just wrapped it in another layer of capitalism with its insurance market.
I tend to agree with majority of this but it’s another can of worms altogether. It’s also an alternative reality nowhere near existing. In reality, no profit means no healthcare at all so these happen to be important considerations.
Capacity is generally limited by staffing, not space or actual beds. When hospitals report how many "beds" they have available, they're generally not talking about the furniture.
They are absolutely talking about actual physical beds. The bed is licensed by the state and inspected by a regulator and is an indication of how many patients can stay in the hospital. As as been shown these years, they can and will pay what is needed, finding qualified people is the hardest part.
Maybe to you, but officially you have 200 beds at 50% occupancy. If needed, nurses can be added by other means. For example, the army, FEMA, etc. will ship in nurses and just need to know if the bed is physically there and certified for use.
Do you actually know what you’re talking about or trying to argue towards what a view you “feel” is the right thing?
I happen to work at a healthcare company that reports number of beds and did receive FEMA sourced labor during the pandemic in some of our rural hospitals that were short staffed and literally do not have the physical labor pool to tap into.
I think you’re discussing how you like to interpret the metrics of beds and occupancy but it’s not how it’s actually discussed in the industry.
ED nurse here. Of course n=1: "can be added" doesn't means "will be added". Our ED regularly boards admitted patients to the point we have a single resuscitation room left for new patients checking in or coming in via EMS. Plenty of rooms and physical beds in the hopsital, and by official metrics hallway beds are counted in "beds available". We did have National Guard present for some time, but it was non-clinical warm bodies to sit with patients on suicidal precautions, stock supplies, etc. No extra clinical staff. Though they were incredibly helpful and lightened the load, they did not enable more beds to be available.
It makes sense to the $250k/year hospital chief bureaucrat (not a medical person) and the Pres. and board accept that the extra contractor pay is just short term.
It was great for revenue. Hospitals got paid for using Remdesivir, which has no approved medical use anywhere worldwide and had a test on Ebola virus patients halted because it was killing faster than the Ebola virus.
https://www.cms.gov/medicare/covid-19/new-covid-19-treatment...
' October 22, 2020, the FDA approved remdesivir (Veklury) for the treatment of COVID-19 for adults and certain pediatric patients requiring hospitalization '
It doesn't even work for helping recovery. Literally poison with no medical use anywhere for anything. Another drug company and hospital emergency payday.
Can't edit my other comment but also wanted to note that they added the clawback provision, which is a common tactic. What this does is allows them to add any type of payment scheme they want, and they can decide later if it was abused. So, if medical professionals are prescribing a drug with no medical value, they can decide that was fraud later and recoup the funds. It may be 5 or 10 years later but they often do this type of thing, hospitals are aware of that risk, and it would be rather cavalier/criminal to significantly abuse it for financial gain. It could even result in criminal charges, lost medical licenses, etc.
It’s hard to tell but these things have been rolled out quick with a broad approach of; don’t give any hospital any reason not to admit a sick patient during the pandemic. Normally a patient in outlier territory would have a hard time finding a long term acute care location if they were likely to lose the LTAC money. So they quickly instituted various add on and kicker “bonuses” such that nearly no patient would loss the LTAC money.
LTAC companies, in capitalism, would simply not accept patients if they thought they were too sick to make money on. Accepting parients put them out of business. The government wants hospitals to admit as many patients as they can in a health crisis. So , I feel this was more of a case where they acted quick and broad and didn’t actual think much about whether the drug was valid. If doctors want to prescribe it, it shouldn’t bankrupt the hospital where they work. The clinical value is up to the medical professions to figure out.
From a Canadian stand point you American nurses are already highly paid. My brother works in the US and was recently thinking of coming back to work closer to where he grew up. The best deal he could get here was $20usd less then what he makes there. So on top of making $20 more then a nurse here he is also making it in USD. He is making huge amounts of cash as a nurse down there. How much more do nurses need?
What you need to realize is that nursing salaries in the US are NOT uniform. From what I've seen in past discussions about it is they range anywhere from $20/hr -> $100k/year. The $100k/year are usually achieved only in cities and generally only by travel nurses.
The majority of nurses, that I've seen, are clocking in at 50->60k yearly salary.
Sort of like saying "Oh, that google dev makes $300k a year. How much more do devs in the US need?"
> Sort of like saying "Oh, that google dev makes $300k a year. How much more do devs in the US need?"
And the answer to that is "how much is Google worth?" If your business relies on the efforts of software engineers to design and build your primary products, they should have the primary equity in the company. So no, even Google developers aren't paid nearly enough...and they're certainly overworked, regardless of how much they make.
> relies on the efforts of software engineers to design and build your primary products, they should have the primary equity in the company.
The average tenure at Google is 4 years. This means that most current Google's have joined when the company was already at sky high valuation. They made incremental improvements to the product line. But arguing that they should own the majority of the shares is just ridiculous. Think about it: if google had made no new development in the last 4 years, how much would it still be worth ? The answer is: not as much as today, but probably quite a lot.
Current employees thus deserve a part of the pie, as they are the one tending for it. But when they joined the pie was already very nice, and they had 0 impact on that. Not with their work nor their investment, so they can't claim that part for themselves.
The nursing labor market is so fluid, so much turnover, it operates much more like a commodity exchange where prices are concerned. This doesn't apply to people to refuse to change employers so incentivizes short term rate chasing
Nursing, just like many other social oriented professions, attract a lot of people for the right reasons, like wanting to help other people, yet too often that well-meaning motivation is then exploited to the maximum by overworking and underpaying these people.
They will bear a lot of that, because these people care for their patients and leaving a job because of bad circumstances also means leaving their patients behind with those bad circumstances.
Which is not something that comes easy to everybody who makes "helping others" such a big part of their work motivation.
Canada is generally more expensive and taxes more (especially when you factor in sales taxes and such).
To be honest, I am amazed that Canada has a healthcare system left.
Decades of mismanagement and underinvestment aside, almost any Canadian healthcare worker can cross the border and instantly see a substantial pay bump and increase in QoL.
I do imagine within the next 20 years, Canadian healthcare is going to look vastly different. Like something from an emerging market, where sure there is universal healthcare, but you generally avoid it if you have the means.
Something that should always be considered is US healthcare is an expensive nightmare. Public healthcare is a HUGE benefit that I think a lot of outside of US people underestimate. (And no, nurses don't get free healthcare from their hospitals. They have the same terrible insurance everyone else gets).
For example, I have to pay $9000 a year BEFORE my insurance starts covering healthcare costs. (at $5000 my insurance starts paying out and I owe 10% of the bill). My insurance does not cover medicine costs at all.
They are looking into getting nurses from the Philippines and Africa. Works for the UK maybe but there's a huge language barrier for the rest of Europe.
A friend of mine is working in bern and his salaray is 7400 franken. Minus taxes that are nothing (10% or so) and health care ( insane 120 franken.. i pay 600€ in germany) there is much left. Apartments are around 1000-2000, food etc is another 1000… blablabla point is he can safe much more money per month than more german workers make after taxes.
My partner is a physician in an ICU and a lot of her colleagues have talked about leaving the field as well. Their complaints are #2 & #3 along with:
5. Pay cuts - Most of the critical doctor specialties (ER, ICU, primary) that were the backbone of the pandemic got "raises" that were less than inflation (hers was 1.5%) while profitable elective specialties got big raises. The root cause is the billing system where elective surgeries bill pay out more than critical roles. Still, it's extremely demoralizing to be called a "pandemic hero" and have your pay get cut.
6. Criminal and Financial Liablity - Healthcare is delivered by a team yet the financial and criminal penalties for mistakes are assessed at the individual level. Recently a nurse was given a criminal sentence for a drug mistake which many believe was systematic failure (bad UI / IT systems, bad hospital practices, AND negligence on the nurse). Imagine getting sued or jail time as an engineer for dropping a production database. The few malpractice cases my partner has been involved in, it was very clear that the issues were systematic and perpetuated by hospital practices. However, if they had gone to trial, an arbitrary worked would d have been sued and the hospital wouldn't change its crappy practices. Institutions have effectively dodged liability in many cases.
7. Chronic understaffing and burnout - most ICUs have been understaffed throughout the pandemic. From an economics POV it seems crazy that their is a labor shortage but salaries are effectively dropping.
Thank the hero of Medicare, Lyndon Johnson. When CMS actually needed to start pricing things, he directed them to his old buddy, the famous heart surgeon, Michael DeBakey. DeBakey sent a couple fellows of his to DC to write up the price list for CMS. Shockingly, surgical procedures got a lot of money and office visits got approximately nothing. This has propogated for 60 years now with increasing precision as the rate of inflation gets applied over and over. A WAG of "10,000 for bypass" is now "57,348.32 +/- 343.43" but the error represents the uncertainty in inflation over time, not any better resolution on the cost of the procedure.
Why are you so quick to assign blame to the first actors? This expectation that the first people to do something need to make it perfect in every way is completely toxic and one reason for the total paralysis of America.
The majority of the blame here lies with the thousands of politicians, bureaucrats, and administrators who haven't reformed the system in *sixty years*. Not the people who were doing their best with much less information than their successors have had.
I can only hope you feel the same way about a 2nd Amendment written when a single fire musket that took 10-30 seconds to reload was the peak of "arms". 5th Amendment "Papers" could use a bit of rethinking too.
There are a lot of first actions that need to be reexamined in the 21st century.
In relation to #5 we had to drop pay by ~6-7% due to medicare cuts in 2021. Me and my MDs salaries are paid directly from medicare ( and other insurance companies who peg their compensation to the medicare rates ) so we have no choice but to drop salaries or close up shop.
With the inflation numbers this year I have no idea what we are going to do, since we are already 6-7% in the hole from the 2021 cuts and now inflation is 8-9% ( assuming the economic numbers are correct... )
Concierge care/Direct primary care or start your own surgical center that takes cash. My company contracts directly with fixed price surgical centers for elective care and bypasses insurance completely.
> Patients in COVID have become downright mean. Add this to the problems nurses have management and doctors (who are often rude and arrogant) and it's a poor culture.
So...this is also the biggest reason (besides lack of pay or basic human dignity) that restaurants and retailers are having a lot more trouble finding employees. Rude (and sometimes violent) customers were already an issue, but they've become absolute animals lately. It's increasingly bad for your own health, mentally and physically, to have any public-facing job. In the last few years, we've let go any pretense of expecting people to be civil and reasonable, and adult children are rewarded for their behavior instead of being trespassed.
Teachers are also quitting in droves (and in the middle of the school year, in some cases) for the same reason. Children are awful and the parents are worse. You risk sickness and violence, and are constantly harassed by parents. Then there's the whole attack on the curricula and book banning...
The FAA reported 1099 incidents with unruly passengers last year, up from a normal 100-300 in prior years. Because some sorts of people simply won't do what they're told...and disobeying flight crew instructions is generally a federal crime.
Everyone's increasingly overworked and underpaid, and they have to deal with degenerates like that daily. Of course they want out.
Everyone thinks that their belligerence makes them Sam Adams or Gandhi rather than just the jerk they likely are. I see this every weekend at youth sporting events. I'm just like, "it doesn't matter why -- if the ump says you need to leave, just leave -- this isn't Game 7 of the World Series".
Those unruly passengers are frontline help desk that had to deal with a elementary teacher that had to deal with kids that had to deal with parents that had to deal with unruly passengers. Everyone is on edge because scarcity is making a comeback, and we are all paying that stress forward.
I like that view. Most things are shit nowadays and everybody is sick of it. You get pissed on, and then you piss on somebody else because why wouldn't you? Nobody is caring for you, why will you spend the little amount of mhntal resources you have left to care for someone else?
It's toxic but it's the direction the world is moving to as long as the people in power keep choking their underlings and taking away every piece of joy they ever had.
You're right that there are definitely opportunities for improvement here. As a Product person that has worked in EMR/Healthcare IT systems, I can tell you the biggest challenge is most of the decisions are driven by legally-required compliance. In many cases, you literally cannot make it better because the brokenness is /by design/ to comply with the law.
Nearly across the board, especially in the US, our legal and regulatory climate has not kept up with technology and often actively works to the detriment of technical innovation and improving our systems.
I'm in this business too, and it's not just the direct features supporting the law, its the law driving out time and talent trying to make things better. We don't have time to improve systems because we are all too concerned with meeting the latest regulatory pipe dream of interoperable systems.
Systems that nobody has ever asked us to use. Entire APIs with full access to key data, that nobody uses.
Yes, this is probably the bigger impact, to be honest. Teams have limited resources and more and more of it is cannibalized by regulatory compliance work.
We've created so much regulation that no one person can know it all - not the legislators, not the agents/bureaucrats, not the judges, and certainly not the workers or patients who would be most affected by them.
I was just on a 40-person call with Micky Tripathi today. I was on a gov-only call with his minions yesterday. They mean well, but they're policy people, they don't promote by repealing policy (remember, the boss promoting them wrote that policy). No programmer will stoop to a government salary to clean up the mess. Something has to give, and we've decided to break the doctors and nurses until the patients die. Things might change once a few major city trauma systems implode.
Keep in mind, the boomers are retiring and there aren't enough Gen X to replace them. Here's the graph of job postings for my specialty (takes a bit of finagling for it to render, esp. mobile, but suffice to say the system is going bonkers): https://www.pathologyoutlines.com/jobs?jbl=1
HITRUST certification is the most demoralizing thing I've done in my life. You need a policy, a procedure and evidence of things like this:
Shared system resources (e.g., registers, main memory, secondary storage) are released back to the system, protected from disclosure to other systems/applications/users, and users cannot intentionally or unintentionally access information remnants.
I understand exactly what you mean, but having done HITRUST CSF certification for a system, I will say that it is not as bad as some others, because at least HITRUST is /very/ clear in its requirements, so there's not as much vagaries and back and forth with auditors after the fact, or rushed changes. It's truly a nightmare to meet, but once done you can be assured you will pass the audit fairly.
Yep, try doing that in an electron context and you quickly learn why a lot of this software still runs on mainframes with UX from the 80s, hard T1 lines (if they’re lucky enough to be off ISDNs), faxing things all around since that’s considered “secure”, etc etc. A lot of startups can’t touch this stuff due to regulatory hurdles. When the first step is “go change the law”, it’s a non-starter.
I mean, if it was really a very high security system, ensuring that confidential info in memory cannot be written unencrypted to a swap file, does seem like a reasonable requirement.
There is a reason why these things are like this. Someone with influence is making money hand over fist with the current state of affairs, so it says. Regulation are always penned by those in industry they are set to regulate with government connections. Politicians don't do anything unless there is a push for it by lobbyists or donors because that's where the incentives are.
And what sucks about this entire situation is even if you today fixed healthcare, because you havent fixed regulatory capture it will end up screwed up in some other direction as soon as the grifters finish planning out their graft and ringing personal phone numbers in washington DC and state capitols. Fixing regulatory capture is therefore required to solve the big problems we have, like climate change, housing, and healthcare, otherwise no fix will ever be long term and meaningful. The incentive structures with regulatory capture favor personal profit over public good every time.
Doctors and hospitals control some of the more powerful lobbying groups in the United States making it a bit strange they haven't worked on those issues.
> Doctors and hospitals control some of the more powerful lobbying groups in the United States making it a bit strange they haven't worked on those issues.
Doctors and hospitals are not necessarily aligned groups (either with each other or with nurses) on the issues, and private insurers, state governments (as market participants themselves, via operating public insurers such as Medicaid agencies), and other players are also very powerful lobbies.
I think this is looking at the problem wrong. The problem is that implementing positive change in these systems is impossible for reasons far outside the control of any product designer or developer currently on the team.
This software is old, has byzantine requirements, probably cut costs all over the place, and conceived in a board room without the benefit of an adequate development lifecycle or stakeholders advocating for the users.
It probably takes 3 months to move a button around, and instead of moving that button executives are having them push a feature that earns a few more million, or a feature that the customers want more then a UX improvement.
>executives are having them push a feature that earns a few more million
I've worked here before... Half our customers are complaining about feature X that doesn't work right/ is inconvenient. Exec: we don't care they are already paying us on a 3 year contract. Hack this new feature into the program that a potential new customer wants.
Horrible places to work they are. Thats why I avoid using any long term contracts like the plague. The second I see call for pricing I close the window.
> I think this is looking at the problem wrong. The problem is that implementing positive change in these systems is impossible for reasons far outside the control of any product designer or developer currently on the team.
A developer working on something is different from a product designer. For product designer I don't mean a UI/UX developer. I mean someone empowered to design the thing. This is often a leader or product manager.
Product design isn't something taught well in most schools. It's often out of sight and mind. An engineer who was good at building hardware or writing code didn't learn the skills needed for product design through that. Product design requires looking at the whole system differently.
> It probably takes 3 months to move a button around, and instead of moving that button executives are having them push a feature that earns a few more million, or a feature that the customers want more then a UX improvement.
A better UX would reduce the amount of time nurses spend using these systems. That productivity could be used to do more other work (like taking on more patients). I don't like this argument but it's easy to make in terms of cost effectiveness.
I don't think the cost effective conversations are happening. I expect there isn't that level of depth to these. It's hard to do when a purchasing organization (like a hospital) only have a few options and they are all bad.
This is an opportunity. To build software that is both compliant and has a good UX. There's an opportunity to disrupt all the crap software here.
> This is an opportunity. To build software that is both compliant and has a good UX. There's an opportunity to disrupt all the crap software here.
The thing that everyone is overlooking here is that EMR software is not designed with patient outcomes as the top priority. Every single EMR software I've seen in the field has been designed with BILLING as the top priority -- everything is organized around making sure that you can bill for the maximum number of services.
I don't think this can possibly change without regulation. The incentives are all wrong at every other layer.
It is true that billing is a priority and there are profit incentives at work. That's exactly why it's worth it for hospitals to improve the data entry user experience!
Better documentation means more revenue. If your doctors and nurses are not filling in the forms because the interface isn't user friendly, you're losing money.
This is not actually the way the system works, as currently designed, and so correspondingly this is not how EMR systems are designed. The documentation that matters is capturing the procedure codes and inventory codes for billing -- and EMR systems and the associated hospital workflows and security mechanisms are designed around making sure that those billing codes must be entered in order to do anything else.
I asked one of my Smarter Dx colleagues who's an expert on this subject to clarify, and he had this to say:
> There are 2 types of billing, even for hospitalized patients. FFS and DRG based payments. Fee For Service does depend on capturing those billing codes correctly. But DRG based payments depend solely on documentation and the billing codes are irrelevant. FFS is 2/3s of US health care spend currently ($2.6T) while DRG is $1.3T.
I think what you're describing as the Product Designer who can get shit done would need to be at the VP or C level to actually accomplish this within an enterprise organization.
> I don't think the cost effective conversations are happening.
I think it would take years to overhaul these products and the conversations on that and how the price would roll down hill to the healthcare organizations have happened, and been summarily shut down.
I also think startups have tried to sell software via this value prop but have not managed anything close to feature parity or sales-org-maturity as the dominant enterprise players.
> This is an opportunity.
I think various startups and other organizations are trying but there is a reason enterprise-style organizations exist and dominant their various verticals.
Its not only about a good product, its about navigating painfully expensive sales cycles of multi-year or even near-decade, political wheeling and dealing at the municipal, state, and federal levels, dealing with compliance and legal liabilities etc.
> This is an opportunity.
Is it though? Hospitals still run. Yeah its expensive as hell, nurses are quitting, but I don't see the horsemen of the apocalypse quite yet. Healthcare outcomes are ok-ish. Young people are still entering the medical field as a viable profession.
> A better UX would reduce the amount of time nurses spend using these systems. That productivity could be used to do more other work (like taking on more patients). I don't like this argument but it's easy to make in terms of cost effectiveness.
I don't think the companies developing the software care, because they're getting paid either way.
I think this might be more of a symptom of administration being detached from the work on the ground. Even if one app had UX that was significantly better (within the realm what's possible within regulation. Others here make the point that the laws and regulations make the UX unregenerate bad), the sale might highly likely go to the solution that has more checkboxes filled in the feature table.
Agree with all of this, and just to add one thing: liability.
Look at the RaDonda Vaught case or the Michelle Heughins case; terrifying to be looking at jail time for a med error.
Many nurses are watching these cases more closely and deciding that since staffing isn't getting any better and they won't be protected, it's not worth the risk.
That case goes far beyond med error and I don't understand why people keep bringing it up as an example.
She pulled the wrong med, and then injected it and walked out of the room rather than observing for effects. Also the med she pulled had warnings on all sides of the bottle and on the top saying very clearly that it's fatal to administer without ventilation. This went beyond a mistake to negligence.
Janie Harvey Garner, a St. Louis registered nurse:
“In response to a story like this one, there are two kinds of nurses,” Garner said. “You have the nurses who assume they would never make a mistake like that, and usually it’s because they don’t realize they could. And the second kind are the ones who know this could happen, any day, no matter how careful they are. This could be me. I could be RaDonda.”
> Also the med she pulled had warnings on all sides of the bottle and on the top saying very clearly that it's fatal to administer without ventilation.
The linked PDF includes images of medicine in question. There's a single warning on top that reads "WARNING: PARALYZING AGENT" and a red cap. I don't see any warnings on the side. The vial appears to be tiny, smaller than my thumb.
But yes, she made a series of mistakes, listed on the last two pages of the PDF.
I am not a nurse, but I can easily imagine how someone could make the errors she did in an overworked and high-stress environment. It's a cascading series of errors that starts with overriding the medicine cabinet when she can't find the medicine she's looking for. But according to her defense, overriding the cabinet had become almost standard operating procedure at Vanderbilt at that timeframe. Once she starts down this path, she's operating on automatic and almost blind to what she's doing.
I agree she was negligent. I don't think she should go to prison for it. In the bigger picture, this is causing more nurses to quit, likely leading to more medical errors and deaths, not fewer.
> I am not a nurse, but I can easily imagine how someone could make the errors she did in an overworked and high-stress environment.
There are so, so many differences between the two meds, I don't see how confusing them would be possible short of gross negligence (for context, I am a paramedic, and often administer medications (including both of the meds involved here) in a high stress environment).
Vecuronium (the paralyzing drug) is a powder in the vial and you need to first inject saline it into the vial, shake it up, and then draw out the "reconstituted" med. This is very unusual (there are only a handful of medications in common use that require this, and Midazolam, the intended med, is _definitely_ not one of them). The reconstitution process means she would have had to look at the top of the vial several times, and warning on the tops of vials are, again, very uncommon. Also uncommon is the red cap on the vial.
I have made errors before while caring for patients, and I will likely make them again. I am very aware of the fact that we all can make mistakes, but the number of mistakes that needed to be made here far exceeds the standard of what is reasonable, and is well into the territory of "gross negligence", in my opinion.
I appreciate your perspective as a medic. The PDF I linked enumerates the mistakes she made and the differences between the two medicines, and I have read all that. From non-professional perspective, it seems like it was inattentional blindness.
But let me allow for a second that this is a case of gross negligence, despite the fact that CMS investigated Vanderbilt and found many other issues in the workplace:
It's not clear to me how criminalizing her mistake helps prevent future medical errors. Do you think criminally prosecuting her was the right decision?
I am neutral on the idea of criminal prosecution here (for the individual, I absolutely thing there should be accountability for the organization). I am generally opposed to criminal prosecution for medical errors, but it's hard to overstate how outlier this series of mistakes was in terms of the severity of the outcome and the degree of negligence demonstrated.
I think the question of "should we put this person in prison for these actions" is equivalent to any other criminal act (which isn't a clear cut answer either, in my opinion).
Yes we do, but we also give DAs discretion over when to enforce it. Given the extenuating circumstances, I don’t think it should have been enforced here.
Her employer, by not creating a culture of safety, set her up for failure.
I just don't see how in the long term this prosecution reduces medical errors and generally disagree with criminalizing mistakes; even ones such as this.
Enforcing criminal liability for homicidal negligence is how you force respect of even basic safety requirements that already existed.
I'm not arguing that hospitals aren't currently a shitshow, I'm aware I've worked in them. That doesn't excuse this nurse's complete lack of respect for the risks she took.
As I've said before, if aviation insisted on criminal punishment for pilots, we'd be far worse off. Many accidents are caused by fear of punishment. Culture of safety can only be implemented and enforced top-down. Why punish the nurses when they're not the ones responsible for what kind of culture exists at their institution?
We do sometimes punish pilots criminaly. For example one easy way to go to prison is trying to fly a plane under the influence of alcohol. (Here is an example [1])
We do not punish criminaly pilots for other kind of mistakes. For example you are unlikely to go to prison if you miscalculate the required fuel for a flight.
I don’t know the details about the nurse. Was it more like the first or more like the second?
I don't particularly care about the nurse being mentioned or the details. I'm far more concerned about the fact that nobody seems to be interested in talking about or making regulatory/process/culture changes at this hospital and/or others to ensure that it can't happen again. It's too easy to make individual nurses responsible for deaths when the actual cause is in the processes that allowed it to happen. I'm not seeing this kind of investigation. Where's the FAA/NTSB equivalent for healthcare?
That enforcement causes nurses to not want to work, as the nurses aren't the decision makers in making a culture of safety. The administrators bear that responsibility so maybe we should enforce it on them.
This nurse was the decision maker in whether she bothered to check the label on the vial for what she was injecting to the patient, and / or bothering to scan it as required before leaving them to die in terror.
I'm not sure what world you live in, but I'd like to live in the one where criminal negligence resulting in avoidable death is prosecuted.
If nurses quit over criminal liability for killing someone by being that careless, everyone is better off by them not being in the field. Pharmacy has had the same rules for over a hundred years. A great example is even in the movie a wonderful life.
If you don't go to jail for this, do you do so for any sort of negligence? What about an Uber driver that runs a red light and kills a pedistrian walking? Or is drunk and kills someone? That worries me a lot more than this story.
Literally every medication has warnings slapped all over it. My partner worked at Vanderbilt (on a different floor) around this time, and one constant complaint I heard (prior to the incident) was how there was hardly any controls around anything there.
Every medication does not have a bright red cap with a bold warning printed on the top (that you have to look at at least twice while reconstituting and then drawing up the med). The warnings on a vial of Vecuronium go well beyond the typical "This medication may case XYZ side effect", and for very good reason.
Yeah, there's no doubt that this is a shitshow from how Vandy is described (and nursing in general especially with these automated pharm boxes), but that should be additional consequences, not this nurse avoiding hers.
The hospital that hires the nurse should be responsible for the nurse. Period. Under all circumstances.
The hospital has far too many incentives to play fast and loose and then leave the nurses in the lurch with a system stacked against them. The hospital has far too many incentives to skimp on training and safety. etc.
Should this nurse also have her license looked into? Yeah, it looks like it. And is it up to the hospital to fire her or not? Yes.
However, barring actual proof of premeditation, all charges and fines should land on the hospital--not the nurse.
My GF is a nurse and I've heard her talk about working a number of 12 hour shifts and not having the ability to go to the bathroom, get water, or have lunch, all because of how strapped the unit is and arduous the requirement is to do these things (usually having to leave the unit). I'm honestly shocked we're not hearing more mistakes, and it should be 100% hospital admins on the chopping block for forcing these insane work environments upon nurses while expecting quality patient care.
People like you are part of the problem. "It was covered in all kinds of scary warning labels"—just like every other medication in that drawer. Medical professionals are totally blind to alerts given off by their EMRs because everything has a password-protected warning so that the audit logs can say "yes, this physician/nurse read and understood the warning"
No, very different from every other med in the drawer. The red cap on the vial is very unusual (reserved for very dangerous meds like this), and the bold printed warning on the top (that you have to look at at least twice while while preparing to administer this medication) is also something used very rarely.
I believe you can even be personally liable for HIPPA security violations as a user or dev of a healthcare system. That seems a bit scary. I agree that regulation persuades people not to do things out of fear of breaking the law. We see this in it's intentional form with regulation of other things such as abortion, guns, etc. Put so many laws in place that risk of accidentally breaking one and receiving an extensive punishment isn't worth it.
> I believe you can even be personally liable for HIPPA security violations as a user or dev of a healthcare system.
Welcome to being an engineer, if that's what you want to call yourself. The engineer who approves a bridge design can be held liable if it collapses due to a design fault.
One difference is that HIPAA has a bunch of statutory penalties for "technical violations" that might or might not harm anyone. For example, if a call center staff discloses patient information to, say, the child or parent of a patient, that comes with an automatic fine and (potentially) jail time.
Another aspect is that certain HIPAA allowances for data usage require a lawyer's expertise, not an engineer's. For example, can a health insurer use patient data to train a model w/o first obtaining patient consent? If the model will be used for "healthcare operations" (i.e., adjudicating claims), you might argue that the answer is yes. If the same model will be used for suggesting treatment options to doctors, you might argue that the answer is no. If you answer wrongly, you are hit with a statutory fine.
It's like having a fine for painting the bridge the wrong color because there is a law that bridges must be green, but you used lime. Not because you're worried about the bridge collapsing, but because the law says so.
Generally, civil engineers don't need to worry about fines or jail as long as things stay up.
Generally the firm's insurance will cover an engineer since they are a "professional". Software "engineers" generally have not been individually liable for bugs. Usually the software user agreements don't allow for this sort of thing.
Basically, contracts can control the liability in most cases, but HIPPA prevents that by explicitly defining liability under the statute.
Lot's of better paid gigs with better working conditions where you aren't personally legally liable if you write a bug. I don't especially care about what job title some board thinks I'm allowed to use.
Yep. I believe that's really the core of the article - overhead like regulation and liability on top of working conditions have people looking to other professions.
Married to an RN and absolutely sympathetic to the staffing/pay plight they're currently facing. I'm unfortunately not very familiar with the case of Michelle Heughins, but I've heard a lot of the RaDonda Vaught case. The high points of the case as I understand them:
* Vaught stated her department was not understaffed, nor was she tired. The incident also occurred in 2017, so pre-pandemic
* Vaught went to dispense Versed (generic name midazolam) by the brand name, instead of the generic name as they're trained to do. This led to her selecting vercuronium bromide instead
* Vaught stated she had dispensed midazolam several times before, which would have had to have been by the generic name
* Vaught ignored several warnings from the dispensing machine stating the patient was not prescribed vercuronium bromide
* Vaught ignored the red cap on the vial dispensed that stated it was a paralytic agent
* Vaught ignored that vercuronium bromide needed to be reconstituted with sterile water (unlike midazolam, which comes as a liquid). She stated she thought it was odd that she didn't have to reconstitute it before when dispensing the correct medicine
* Vaught did not scan in the medication before or after giving it to the patient, which would have likely prompted another warning about it not being prescribed
* Vaught could not recall exactly how much she gave to the patient
* Vaught immediately left the room after injection, and did not wait to observe the patient for any side-effects
The opinions on the case I've observed have been nurses who aren't aware of this and saying she should not have been convicted, and the nurses who are aware who think the conviction is fair ...ish. The latter is at least unanimous she should have her license revoked.
Most agree that Vanderbilt should be held responsible for negligence as well. My wife's hospital for instance does not stock _any_ paralytics within machines, to prevent it being accidentally dispensed without involving the pharmacy. There's also evidence that Vanderbilt tried to cover the incident up.
I've made a point of stressing to any RN I've talked about it with the importance of having a lawyer with you when talking with investigators. Vaught straight up incriminated herself multiple times during her initial interview.
I'm not familiar with the case, but assuming what you've outlined above is accurate, I have no doubt a jury would convict. Negligence actually sounds like too nice of a word for that train wreck of events.
Don't forget that nurses can now legally be thrown under the bus with criminal charges for malpractice while hospitals walk away scotch-free [1]. This is huge in the nursing community right now.
This kind of thing is going to further disassociate nurses from interacting like a human with their patients. If you risk criminal prosecution and prison time from making a mistake, everyone starts walking on eggshells and become afraid of doing anything beyond box ticking. They'll start turning a blind eye to things they know are wrong, because the system doesn't see them. All work will align towards pure compliance with the law and the hospital system at the expense of intimate connection with patients.
And of course, a lot of nurses are in the job for the human connection, and will consequently be burned out at an increasing rate.
To some degree this might actually be good long term, because it will be that much harder for hospitals to manipulate nurses into working around the limitations of the system to provide real care, which allows the administration to turn a blind eye to their own flaws. There's going to be a surge of malicious compliance that ends up shining a bright spotlight on just how abusive and dysfunctional hospital systems really are.
And patients will ultimately be the ones who suffer.
> Don't forget that nurses can now legally be thrown under the bus with criminal charges for malpractice while hospitals walk away scotch-free
The nurse in that case was prosecuted for criminal reckless homicide (not malpractice, which is civil negligence.) The characterization of the hospitals direct responsibility is negligence not arising to criminal (gross) negligence (as the principal of respondeat superior doesn't apply in criminal law, the employees recklessness would not be imputed to the employer the way it would in a civil case.)
As for civil liability if the hospital, that was settled out of court with the victims family, the hospital did not get off scot free.
This... isn't a new thing that deserves the “now” label like it is a change. Criminal wrongdoing by employees (including in healthcare) very often does not rise to a level of criminality for the employer, and that's been true for a long time.
You aren't wrong but you also aren't giving my comment the benefit of the doubt. I'm not a lawyer. When I say "malpractice" I'm not referring to the legal definition of the word, but the layman's term, defined as, "improper, illegal, or negligent professional activity or treatment, especially by a medical practitioner", which fits here well.
>This... isn't a new thing that deserves the “now” label like it is a change. Criminal wrongdoing by employees (including in healthcare) very often does not rise to a level of criminality for the employer, and that's been true for a long time.
Of course criminal charges for a patient death cannot be administered on an entity like an entire hospital, I didn't mean to insinuate that. But those who share responsibility for her actions: the administrators, doctors, morticians, everyone involved in designing the processes which led to this disaster and being involved in covering it up (i.e. the "hospital"), all seem at least partially liable if we are looking at this mistake through a criminal lens. Would you agree?
Some studies say that medical error is the third leading cause of death in the US [1] - yet how often do we see "criminal reckless homicide" brought against nurses? There was an incredibly disingenuous serious of mistakes that had to happen for this nurse to mess up so badly, don't get me wrong. But when nurses are working 50-70 hours a week doing 14 hour shifts under extremely high pressure from management, these insane strings of mistakes are simply going to be an occurrence, and we shouldn't be using our tax dollars to pay for shitty lawyers to go after them for these mistakes. It's a waste of everybody's time, energy, and money, is detrimental to patients, and is a contributor to the fact that 90% of nurses are considering leaving the profession.
The solution isn't that Radonda Vought, who killed a patient through a string of crassly negligent actions should walk free - one would like to see the whole chain of command be given serious prison time. It's clear that patient safety at Vanderbilt isn't a priority - training and safety culture reflects that.
Strange to see that HN, which is generally suspicious of copaganda, falls for very transparent nursepaganda.
> one would like to see the whole chain of command be given serious prison time
Absolutely. To each according to their authority.
RaDonda Vaught made a mistake, and admitted it, repeatedly, in multiple interviews.
But that mistake was only partly because of her free will. Vanderbilt University Medical Center incentivized her to make that choice, for their own profit, and with control over her employment.
RaDonda Vaught goes to prison.
VUMC pays a fine and nobody goes to prison.
I think HN takes a dim view of a company holding someone's contract in their hands, saying "Do something illegal or I tear this up," and then blaming the employee when everything explodes.
They're playing chicken with patients' lives, and passing off the charges to their employees when they lose.
The strong libertarian vibe of npr saying she's being scapegoated?
When you have millions of drugs being issued, there will be some legitimate mistakes happening -- some will even cause death. If you want people to actual work in healthcare, they shouldn't be fearing for their lives for being less than perfect.
please cite where an npr report gives the impression she's been scapegoated in such a way that she doesn't deserve the consequences she's been given. I'd love to read it honestly.
From what I've seen there's been a lot of reporting on her case, and how Vandy rightfully deserves a lot of pain, and a lot on how a subset of nurses feel she's been railroaded, but I've not seen what you claim and would like to know where I missed it.
I'll also re note that pharmacists have carried this burden for over a hundred years, and their removal from the process is part of how this chain of mistakes happened to begin with.
"she doesn't deserve the consequences" is different than scapegoating. Scapegoating means she's the sole person being blamed for the failures of a larger group.
From the article:
"pursued penalties and criminal charges only against the nurse and not the hospital itself...Vanderbilt received no punishment for the fatal drug error...appears to support defense arguments that Vaught's fatal error was made possible by systemic failures at Vanderbilt."
That certainly seems to lay claim that there are more issues than the single nurse. Holding others accountable doesn't negate her culpability but it would prevent her from becoming a scapegoat.
But the electorate continues to reward "tough on crime" prosecutors. Their incentives are all towards maxing out the savagery towards defendants, systemic repercussions be damned.
From the article:
> Janie Harvey Garner, the founder of Show Me Your Stethoscope, a nursing group on Facebook with more than 600,000 members, worries the conviction will have a chilling effect on nurses disclosing their own errors or near errors, which could have a detrimental effect on the quality of patient care.
> "Health care just changed forever," she said after the verdict. "You can no longer trust people to tell the truth because they will be incriminating themselves."
That's the exact opposite of how the NTSB operates. It satisfies the infantile urge to blame and shame a supposed evildoer, to the great detriment of everybody in the long run.
> That's the exact opposite of how the NTSB operates.
Bingo! I have a friend in the UK who organizes "post-mortem" (no pun intended) workshops and process training for hospital staff, precisely to do the NTSB-like thing after medical procedure errors occur. Rather than trying to point fingers and identify scapegoats, the central question is: "what went wrong here, and how do we reduce the chances of that happening again?"
Of course, occasionally the answer might be "We hired the wrong person, and we should fire them", but that seems to be only very rarely true.
this is fairly common in the medical field, the usual name for it is "morbidity and mortality" [0]
> The objectives of a well-run M&M conference are to identify adverse outcomes associated with medical error, to modify behavior and judgment based on previous experiences, and to prevent repetition of errors leading to complications. Conferences are non-punitive and focus on the goal of improved patient care.
I don't think "tough on crime" voters strongly differentiate, based on the behaviors of the prosecutors themselves. The biggest resume priority seems to be maintaining a ludicrously high conviction percentage, which is awful for different reasons (innocent defendants forced into plea bargains).
Only a small subset of prosecutors elected in the most liberal districts are rewarded by their constituencies for exercising prosecutorial discretion. I say that without making any judgment as to whether they're using that discretion well — I'm just observing that very few prosecutors work that way.
> I don't think "tough on crime" voters strongly differentiate, based on the behaviors of the prosecutors themselves. The biggest resume priority seems to be maintaining a ludicrously high conviction percentage, which is awful for different reasons (innocent defendants forced into plea bargains).
Well, I think your position is probably one of ignorance. Plenty of people I talk to are for tough prosecution on things like violent crime and against tough prosecution for simple drug possession.
> Only a small subset of prosecutors elected in the most liberal districts are rewarded by their constituencies for exercising prosecutorial discretion. I say that without making any judgment as to whether they're using that discretion well — I'm just observing that very few prosecutors work that way.
Yes, that does seem to be a trend. Prosecutorial discretion is actually important, but it doesn't mean you let crime run rampant, either.
> The biggest resume priority seems to be maintaining a ludicrously high conviction percentage, which is awful for different reasons (innocent defendants forced into plea bargains).
I don't live in a jurisdiction that elect prosecutors, but is this actually a thing? Do candidates/incumbents run campaign ads on their conviction rate? Are voters researching/talking about the conviction rate of the candidates like it's a pissing contest?
> If the conviction rate had been measured by actual cases pursued, rather than all cases referred by police, Hallinan said, his office would have had a conviction rate that was relatively similar to Los Angeles and other major cities.
> And Hallinan was getting results. Overall, crime rates were plummeting. Violent crime had gone down close to 60 percent in San Francisco since Hallinan took office.
> Still, the low conviction rate resulted in headline after headline about San Francisco’s permissive attitude toward crime, a media environment harnessed by the Harris campaign.
Do we really want to live in a society where people are not prosecuted because the family of the victim forgave them? So if two people commit the same offence, Person A is not prosecuted because the victim's family forgave him but Person B is because the victims family did not? Was offender B just unlucky on victim selection? The rule and application of law should not be based on the feelings of the victims family. Did the dead person forgive them?
We certainly don't want to ignore them, given they have the most immediate understanding of the situation and entitlement to guilt.
We don't allow plaintiffs to sue without standing. Why do we allow DAs to prosecute without a victim?
The state has a justification to pursue crime, but it seems like that should be limited when there's (no victim) or (victim who disagrees with prosecution).
Is the dead person not a victim? If someone is murdered and their family is like good I hated them anyway does that nullify the existence of a crime? Are we basing prosecution now on the character of the victim? That's a pretty quick path to deciding that certain victims have no value in society.
The dead person is a victim, and in a perfect society we'd just execute the killer. 1:1.
In reality, the justice system is imperfect, inequal access to defense, imperfect identification of killers, etc.
All murder is bad.
But I'd certainly say murdering a good person is worse than murdering a bad one. And if a family, who on average has more incentive to think well of the victim than anyone, doesn't... should that be ignored?
I hear what you are saying but honestly yes it should be ignored. For reasons of both fairness but more importantly I want justice to be blind. I don't want the police or prosecutors to be able to decide that person A was a dick or was a republican or a democrat or white / black so his murder is not as important. It could also lead to situations where the murder of a rich person is prosecuted more harshly than that of a poor one as the rich person donated so much to charity. The law has to be blind and based on clearly defined parameters.
But I feel like discretionary prosecution is already breaking blindness.
And furthermore, perversely-incentivized blindness. Get a high conviction rate, by throwing the book at people charged with "PR bad" crimes, regardless of the individual, and as long as they aren't politically connected and potentially useful in your future political career.
Compared to that motivation of your average DA / USA, "How surviving family feels" doesn't seem worse.
I agree with you in regards to how the current system is not blind and discretionary prosecution is a negative. I am all for pretty much anything that removes a prosecutors ability to give a pass to a preferred class of offender. By that I generally mean police officers. Giving them an additional power to decide the value of a victim based on their family or their biased opinion of goodness is not a net positive and just further greys the area. I hear what you are saying and actually sympathize with it but I think the solution should be to focus on removing as much discretion as possible as it just gives prosecutors and law enforcement decision making power they should not have.
If the entire chain of command is responsible, but only one person responsible for the poor result pays a real price, then is it really justice at all?
I'm not saying the rest of them should not be prosecuted if there was fault further up the chain as well. I agree they should be. In this case the nurse clearly breached many protocols and delivered the killing action so she bears responsibility. If there is a systematic failure then they should pursue that too. Justice is not a decision that well we could not get them all so no point prosecuting anyone.
Consider this: someone drives without paying proper attention and kills someone. It's time for victim impact statements, and relative after relative asks the court for lenience on the driver because the victim was a drunk and a wifebeater, the world is better off without him.
Not sure that that is a good idea, justice is about more than just those immediately affected by a crime
Is it though? Should a cop be prosecuted for accidentally killing an innocent civilian in the course of duty during a non violent traffic stop? I would argue that they should be. How many chances should a nurse get to accidentally kill someone? Do they only get prosecuted the second time? Third?
If you are responsible for the death of another person due to your own negligence then you should be prosecuted for a crime and be removed from any scenario where you are able to repeat that mistake.
A cop killing an innocent civilian at a nonviolent traffic stop can pretty much happen only because of malice or negligence. We use the word "accident", but it's never really an accident. If a nurse accidentally kills someone, it may really be an accident.
Furthermore, the nurse is in a profession where people die all the time due to reasons beyond the nurse's control, and surviving relatives are not always rational in who they blame. So nurses will be falsely accused much more often than police.
> A cop killing an innocent civilian at a nonviolent traffic stop can pretty much happen only because of malice or negligence.
This was found to be by recklessness, which is beyond negligence but short of malice.
> We use the word "accident", but it's never really an accident.
Acts due to negligence, and even recklessness, really are accidents.
> Furthermore, the nurse is in a profession where people die all the time due to reasons beyond the nurse's control, and surviving relatives are not always rational in who they blame.
Surviving relatives don't make prosecutorial decisions, nor are they triers of fact in criminal cases.
> So nurses will be falsely accused much more often than police.
That...doesn't follow from what you’ve described, even taking everything preceding it as true.
> A cop killing an innocent civilian at a nonviolent traffic stop can pretty much happen only because of malice or negligence.
I'm not sure this is true, specifically because the difference between a nonviolent traffic stop and a lethal (to the officer) traffic stop can be a split second.
If my keyboard had a 0.01% chance of lethally shocking me... I'm pretty sure that would alter my typing behavior.
"can pretty much happen only because of malice or negligence"
Negligence means "failure to take proper care in doing something", which is often just called an accident.
That is exactly what the nurse did, she failed to take proper care and someone died. The nice thing about the law is that what the relatives feel should not matter at all, that's why we are supposed to have impartial prosecutors that review the facts and determine if charges are warranted.
Bottom line, no matter the profession if you fail to take proper care and someone dies as a result, you should be prosecuted and prevented from getting the opportunity to do it again.
>Negligence means "failure to take proper care in doing something", which is often just called an accident.
This is not true, because you're equivocating on the word "proper". An accident is failure to take proper care, where proper care means "care that follows the rules". Negligence is failure to take proper care, where "proper" means "can reasonably be expected". They are not the same thing.
Not really sure where you are getting those definitions from. Proper means proper. The nurse did not follow the rules. The nurse did not provide any of the care that could have been reasonably expected. Fail to see a difference, she failed both of your definitions.
I have training similar to a WFR that I got in Argentina. I wanted to certify as an EMT in California because why not? It's 160 hours of classes plus 24 hours or practical or something like that for the national exam and then it's the state requirements. Private training is around 2000 dollars. Ok I'm cool with that.
There's no way to get a certification with online learning or with any kind of in person time schedule compatible with my job... ok... maybe I can get time off? I have to re-get all sorts of immunizations I already have and re-do medical checks that I already had to get for my green card, like a year ago... ok... that's a lot more time off. Oh, they drug check me! well... I guess even I would work on healthcare more for vocational reasons I'm not doing it while I'm in California. It's just too much of a hassle and with the staff shortages I feel I'm just being taken advantage off.
In Nevada it's only take the course, pass the exam and you can already go on an ambulance, so are most other states.
> 3. IT systems that they have to use were designed by people who have not talked with the workers who use them. They may have been designed with laws and compliance in mind. Nurses aren't the people who choose or pay for these systems. But, they use them a lot (maybe the most) and it's obvious they weren't taken into account when designing the UX. It's maddening for them.
> This one is big for product designers. Often we listen to the people who pay for it and miss out on the people who actually have to use it.
This resonates with me strongly for two reasons. First my mother is a retired RN, and the electronic record keeping was her biggest frustration. It is hilarious to me how much my mother hates computers, while I make a living in software.
Second, I'm now working for a startup, Smarter Dx (we're hiring: https://angel.co/company/smarterdx/jobs ) that works with these records and tries to make better use of them. To the extent that we're successful, incentives are created for the hospital to improve them, conceivably including improving the UX that nurses see. I don't mean to underestimate the difficulty of the problem, but I think it's possible to at least push in the right direction.
Back in the days before cell phones, my mom would wind up being on call for overnight labor & delivery. The final straw (certainly not the first) was that they got a call in the middle of the night that a woman came in in labor, and she had to drive in to work (a half hour drive). This woke up my dad, who also happened to be a light sleeper and worked a day shift.
20 minutes later (while my mom was well on her way into work) the phone rang again- it was a false alarm, she didn't need to come in anymore. Naturally, it was my (not so happy) dad who answered.
By the time she got in, they didn't have anything for her, so sent her back home.
At the time, there wasn't quite such a crunch in nursing, so the pay part wasn't accurate yet, but everything else you listed (substitute COVID for %50+ of patients) was already true 30 years ago.
I would think some hospitals have rooms dedicated for the on-call nurse(s) to sleep in. Especially with something as common and false alarm prone as overnight labor & delivery. Pretty sure the midwifery I went to had this.
3. IT systems that they have to use were designed by people who have not talked with the workers who use them.
You couldn't be more right about that. Last week a nurse had to use a computer in my wife's hospital room to log that she'd given her a painkiller. The IT staff had failed to configure the hospital computers to disable windows updates or restrict them to off-hours and the nurse was forced to stand there for ten solid minutes while Update churned, the pc restarted, and Update churned some more.
I think this is a great summary of some of the main challenges nurses are facing.
I'd add to #1 that travel (temp) nurses are making 4x+ more than staff nurses, I've heard as high as $13-17k per week in high-demand areas. This exacerbates the problem, as staff nurses hear this, and if they can, they leave. Travel nurses can be great, but they won't know the facility and workflows and people as well as staff nurses: staff nurses now pick up more slack, all while getting paid 1/10th what their new colleagues are. This is more than most doctors.
For #3, this problem is made worse by additional compliance burden. Nurses need to document more and more, click more and more, read more and more… with less and less time. And on systems that are unpleasant to use. Among other issues, this leads to problems like these[0], which drive more and more nurses away.
I'm working with a badass team on solving some parts of these problems, particularly relating to technology and workflows. If you're interested (across basically any role, but product designers, engineers, product managers are top of mind right now), let me know (email in bio)!
> IT systems that they have to use were designed by people who have not talked with the workers who use them. They may have been designed with laws and compliance in mind. Nurses aren't the people who choose or pay for these systems. But, they use them a lot (maybe the most) and it's obvious they weren't taken into account when designing the UX. It's maddening for them.
I can speak to this a bit. After interviewing lots of hospital workers, I can tell you that the hospital quality people love EHRs because the reporting functions actually work. Previously, it was not possible to measure how well the hospital was doing and convince the doctors to improve practices - think washing hands before doing examinations.
EHRs are shitty because (1) the big players are entrenched - they are already implemented and the cost / disruption to switch to a new EHR is extremely high, and (2) the market isn’t big enough to justify the level of investment it will take to break through - Apple made more money from one product (AirPods) last year than all the EHR vendors combined.
At this point my hope is that mobile devices and meta-EHRs are able to crack this.
And even within that single country, each state and hospital then has their own requirements around EHRs. This ends up being my biggest issue with EHR is that you need to support infinite flexibility for all the unique snowflakes that exist. I'm convinced healthcare would improve in this country if the federal government standardized all of this to a single setup. This also includes the mess that is EHR in EMS.
> 4. Nurses are the catch all for jobs. Not enough aides? Nurses do the work....
The nurses aides would argue that they do the majority of the frontline work while getting paid a fraction of what the nurses make, and get even less credit.
Most of the nurses I talk with speak about a lack of nurse aides. When there isn't a nurse aide the nurses have to do that work. When I speak of a lack of them I know nurses who can go multiple consecutive shifts without an aide working the floor. When they do work there is 1 aide to a floor and can't cover everyone so the nurses do that work.
>1. Many new nurses make the same or more and long time nurses. It's frustrating when the nurse in charge with the most experience is making less than new nurses. Some hospitals are even trying to stop nurses from talking about pay.
I think non-performance-based pay is something endemic to many female-dominated professions.
My wife used to work in childcare, and it did her head in that she was paid less than complete idiots who'd been working there longer than she had.
I work at a startup* trying to tackle nurse burnout, and two of my family members are nurses. Here are a few things I've learned:
- Nurses were getting burned out before the pandemic, and the US has a nursing shortage that's been going on for about 90 years (it started with an infrastructure buildout in the 1930s).* So it's a secular problem, with chronic as well as acute causal factors.
- There is a ladder of nursing credentials, and the shortage effects them differently. Hiring for roles like CNA and LPN/LVN has exploded because of the shortage of RNs and above. CNAs get trained in 4-12 weeks to do the heavy lifting of care; RNs get ~3 year degrees to perform much more complicated tasks.
- Burnout, and the nursing shortage, are in a positive feedback loop/downward spiral. That is, the more nurses burn out, the more they cause other nurses to burn out. Short-staffed facilities have a very hard time pulling back to normal staffing, because nobody wants to join a skeleton crew. (I know of long-term care facilities where the scheduling nurses (the bosses) are working the graveyard shift because they can't fill it.)
- Many nurses work rigid schedules on 12-14 shifts, and a lot of medical errors happen at the end of those shifts. *
- The hot US job market (Great resignation, great reshuffle) is hitting nursing especially hard; it is very sensitive to external shocks. There are paths to easier work and higher pay.
- Many healthcare facilities and systems don't give nurses flexibility or the possibility of advancement. (One family member will need to quit her current job and come back in a year or two to her current employer if she wants to move up a pay grade -- which is like some tech companies -- but slower moving and lower paying.)
- Many facilities are run entirely on foreign staff (the H2-B visa allows that). And many nurses are imported from the Philippines.
This is a good summary, and it corresponds to what I've heard from friends and acquaintances that are currently nurses (or left recently).
(2) is a really perverse statistical phenomenon, and it's unfortunate that nurses are bearing the brunt of our civic and public information failures. It must be particularly soul-draining to heal someone who resents the single thing that would have protected them the most from needing hospitalization in the first place.
>This one is big for product designers. Often we listen to the people who pay for it and miss out on the people who actually have to use it.
Pedantic, but: I think it's the responsibility of the people that pay for it to talk to the people who use it, and buy the best software.
I have a hard time believing that you can sit a bunch of nurses in a room to talk about the software, and that they'd design and/or elaborate on an awesome UX. Is there an example of that ever working? People have funny ideas about what they want. Homer Simpson's car design is a meme for a reason.
Maybe, but nurses have also used "because covid" as an excuse to engage in some pretty awful behavior. Fathers have only very recently been allowed in the room during ultrasounds, for instance. NICUs only recently started allowing both parents to visit at the same time.
preface: my parents are retired nurses and a big chunk of my family works in healthcare.
It sounds like the issues nurses face are global and do not significantly change across different systems (the system in my country is completely different from USA)
It probably comes down to the fact that this is a human problem and to solve it we must radically change the expectations around care and primarily being taken care of.
There's no technological deus ex machina or amount of training that can change the situation without shifting the POV.
IMO people working in HC are subject to a lot of stress and must be protected at the cost of making it a bit unpleasant for the patients to be cured.
It's such a fundamental foundation of our lives that the system should be calibrated to create the best possible working environment for those who are working instead of moving it toward a customer reviewd activity that focuses on their satisfaction.
I know it can sound unpopular, but receiving the best medical care possible is not a right, it's a goal that more often than not it's almost impossible to achieve, so let's improve the working conditions so that the workers can give their best without questioning too much all the sacrifices that the job requires.
I don't know the US system so well to argue, I can only expand on what I meant: the job of healthcare is not to make people comfortable or make their wishes come true, HC, unfortunately, it's not a democracy.
What I've seen in the past 30 years is a gradual shift towards becoming some sort of wellness centers for disease: patients that complain about other patients, patients that complain about their accomodations, patients that complain about therapies, most of all patients relatives that want to have a say on everything that's going on up to the point that doctors simply do what asked to not waste too much time with them.
And to add insult to injury, all the legalities that made taking a decision virtually impossible without risking too much.
Of course there are situations were malpractice causes more damages than the illness itself and those must be reprimanded, we can't afford to disrupt trust in medicine in any way, but the results should be taken into higher consideration than the opinions.
ER, intensive care and other kinds of "hardcore" department should also be judged differently, just like it happens to military personnel who are not subject to regular justice while on duty.
A lot of the problem starts with the fact that most hospitals in the USA were taken over and are now owned by "Private Equity".
If you know ANYTHING about finance, that should send shivers up your back and also make you realize why this happening with nursing.
Private Equity is where you go to get money if:
• Your business is floundering and no one will loan to you
• Your industry is in the ebbing phase and not growing
• You are ignorant or naive about getting money for business
• You haven't done your due diligence
• Your company is in play for a hostile take-over
Having Private Equity getting involved is always a major Red Flag if not Black Flag.
In general, Private Equity knows nothing about your business norms or markets - they don't care. They are a one-size-fits-all investor and that primarily means "Cut Costs on Everything".
It's very akin to having a lawyer become your CEO (e.g. Sears/Kmart) - it's a omen of VERY BAD things being imminent.
A case in point: the COVID bounties from Medicare for testing, admissions, treatment AND DEATH BY COVID are exactly something that Private Equity would love maximally, dream up and probably try to enact with lobbyists.
> IT systems that they have to use were designed by people who have not talked with the workers who use them.
This was exactly my experience when I worked for a medical software startup. Our (very unfinished) software got deployed in a hospital with no training, no orientation, no nothing, and it was such a disaster that it was a patient safety issue. Mind you, the engineering team had no say in any of this, not that we were even given the chance, and we weren't even aware that the deployment was for real. We were under the impression that the deployment was for testing purposes, because we were aware that the software was unfinished.
It was a breathtakingly poor decision purely on the part of managers (and, frankly, sales) on both sides of that deal and it was doctors and patients who suffered because of it. An absolute nightmare all around and I'm glad to no longer be there.
>IT systems that they have to use were designed by people who have not talked with the workers who use them. They may have been designed with laws and compliance in mind. Nurses aren't the people who choose or pay for these systems. But, they use them a lot (maybe the most) and it's obvious they weren't taken into account when designing the UX. It's maddening for them.
This one is big for product designers. Often we listen to the people who pay for it and miss out on the people who actually have to use it.
This!! I had a friend who retired early because she was literally being worked to death. A big part of that is the hours she spent after hours trying to deal with the new IT system.
Totally and completely agree! I spent hours when hospital I worked for 30 years, made our GI lab use the program for documentation and billing from the OR. It was abysmal. I tried and did the best I could with Cerner, but you can’t fit square peg in round hole- no one designing ever asked those that had the 30+ yrs of knowledge that could have developed a unit or specialty specific program. It just wasn’t THAT hard, but management wanted it to work with what they already paid for!
On (3), Kaiser seems to be the exception to this. Their systems, on the nurse/Dr side seem very easy to use and the connections between different departments work seamlessly. At least, from what I've noticed as a 10+ yr Kaiser patient in the Bay Area.
We make really usable software for nurses, and they absolutely love it. I think the effort we go to is totally unnecessary to achieve that, as - just as you say - most medical software is so bad from a user perspective.
>3. IT systems that they have to use were designed by people who have not talked with the workers who use them. They may have been designed with laws and compliance in mind. Nurses aren't the people who choose or pay for these systems. But, they use them a lot (maybe the most) and it's obvious they weren't taken into account when designing the UX. It's maddening for them.
>This one is big for product designers. Often we listen to the people who pay for it and miss out on the people who actually have to use it.
Thats an interesting comment because I know the main developer for one of the most popular hospital systems used throughout Europe and its popular because its good.
Saying that, I also know there are medical consultants at a world famous hospital who dont really know how to program but because of their position have got their software in use when it perhaps shouldnt be.
I know alot of US programmers doing various medical systems for local hospitals and health care regions with various standards of programming skills.
Like you I also know of people in various roles, from world famous multi millionaire consultants to nurses on the front line. Every team & dept is different. Sometimes its a managerial problem at the top of the health trust, other times its just the team and low level management.
Saying that there is a culture of taking a sicky probably because they see consultants putting private work before NHS work and they see the wages some of these consultants get paid and Google Scholar, PubMed, DrugBank etc keeps highlighting the inadequacies of the teaching, ie they dont keep up to date, some areas appear to be decades behind the science other areas are within a few years of the latest research.
Too much reliance on drug companies when superior non patentable solutions already exist.
>IT systems that they have to use were designed by people who have not talked with the workers who use them.
Interesting thread because this is my current $dayjob! I work for an organization that is both a tech company, and a medical services provider, so we can optimize away the boundary between vendor and customer as far as the software is concerned. My particular area of interest is in providing system programmability that can be exploited by tech-capable clinicians to provide both better patient outcomes and more pleasant provider experience. Basically don't try to have software developers understand every last detail of the practice of medicine. Instead provide a programable platform that's usable by a subset of clinicians.
Poor UX for medical systems is something that has always baffled me. I used to work for one of the major CT system manufacturers (although on the firmware end of things). I never understood why a hospital would willingly pay a seven figures price tag for a medical imaging system that comes with an early 90s GUI.
Ultimately, it is not the radiologists or technologists who make this decision. From a purely technical point of view, modern systems hardly differ from each other, at least as far as diagnosis is concerned. The fact that a better UX means new users need less training and the time between scan and diagnosis is reduced are hardly taken into account when making a purchase decision.
>3. IT systems that they have to use were designed by people who have not talked with the workers who use them.
Every time the computers went down at a friends ER, the waiting room emptied out as the staff were able to use paper forms and just get their jobs done, instead of being forced through thousands of menu clicks and choices that made no sense.
EVERY SINGLE TIME -- Epic or as I call it... the Epic Failure. I always give my condolences to staff forced to use it.
> Food service workers don't want to take food into a patients room... nurses will do it
No idea where you live but in German hospitals I've never been given the food by anyone but a nurse. There are literally zero people/professions besides doctors, nurses, and cleaning staff near patient rooms.
> IT systems that they have to use were designed by people who have not talked with the workers who use them.
I worked at a large emr company and the developers had access to nurses and were required to support go lives a few times a year to support nurses on the floor.
about #3 that ain't a design issue, it's a policy issue. Until healthcare in the US is about maximizing profit extraction by every party involved things will not change.
For profit healthcare is an abomination and a blight on the very soul of this country. If I believed in religion I would say God will judge us very harshly for allowing this system to stay in place for so long.
> 3. IT systems that they have to use were designed by people who have not talked with the workers who use them. They may have been designed with laws and compliance in mind. Nurses aren't the people who choose or pay for these systems. But, they use them a lot (maybe the most) and it's obvious they weren't taken into account when designing the UX. It's maddening for them.
Working in Healthcare IT I can only concur on this point.
For me there's multiple reasons behind this issue :
1. Regulations. First and foremost, IT is here to help/force users in complying to those regulations. So it's the first thing that dictates how you'll develop the piece of software.
Those regulations are mostly written by people that aren't Healthcare professionals nor IT professionals. They are regulations people. So they can't produce something that makes sense for Healthcare people and is even harder to _solve_ for IT people.
And those regulations are updated quite frequently, most often creating breaking changes. So if you want to keep up (and you have to if you don't want people ending in jail) you must work fast, meaning skipping important steps to produce something user oriented.
2. There isn't much money. At least on my side of the Atlantic. This is not necessarily a huge problem because contrary to people at FAANG-like companies, here most people are focused on helping people to help other people, not on their paycheck. But there's so much middle-men taking their cut that in the end, you only worked understaffed with unrealistic schedules. Meaning the only way to deliver something is to take big shortcuts. And again, leaving UX/UI on the side of the road to reach the main goal : being compliant with regulations.
And when I say there isn't much money, it's partially true. When it's about buying a nice startup, there is heaps of cash. Because you need to keep the market as closed as possible. But when it's time to actually invest in making better software, the wallet is empty.
3. There's a weird mindset where in most cases, end-users are simply not considered. At my previous jobs, I always asked to sit with actual users of the software to see how they work and what their actual requirements are. Since I joined Healthcare IT, on the ~20 projects I worked on, there's only one case where I was authorized to do so. On all the other cases, the "IT Project Manager" (whatever this is) just said that they knew exactly what the users needed, even though they never actually worked with them.
And on the project I was allowed to work correctly, instead of the original proposal that was agreed on, based on my observations, I came up with a solution that was much simpler for the users, easier to build for the IT team, so delivered faster and at a lower cost. So the customer was happy and decided to sign a contract for another piece of software at the company. Everyone happy in the end. But it's an exception.
In the other domains I worked on, it seems obvious to everyone that gathering intel from the actual users was mandatory to produce something valuable. Here, management think they know better. They don't.
And honestly I don't see how it can improve since those three points keep getting worse and worse every half-year.
Someone I dated last year has worked on the administrative side of hospitals for years. Her statement was "everyone is hooking up in them, and it's typically
ignored. Unless they use a patient bed, then all hell breaks loose."
> 2. Patients in COVID have become downright mean. Add this to the problems nurses have management and doctors (who are often rude and arrogant) and it's a poor culture. The quality of the environment, from a mental health standpoint, is on the decline.
Mean customers, and rude coworkers? I sympathize, but this is a reality in a lot of industries. I have no reason to believe that healthcare here is worse than average.
It doesn't help that hospital systems tend to be garbage at customer service, so the person's been told to wait an indefinite (but always very long) period without any indication of how long it'll be, and asked to tediously fill out the same information five different times on five different pieces of paper and iPads, all while feeling terrible, before they finally snap at a poor nurse who isn't to blame for their hospital being an uncaring money-making machine with little regard for humanity.
Incidentally, Nurses organized by Finnish labour unions are currenlty planning to quit en masse since they weren't allowed to go on strike. Forecasts indicate we'll have a total collapse of the healthcare system by summer unless negotiators manage some kind of breakthrough in the negotiations.
I've spoken with nurses who've had a variety of other jobs at other types of places. They are consistent in telling me that working as a nurse is a worse environment in the way they are treated.
The example stories they have shared are the type of thing I can't relate to and I've worked in software, general engineering, food service, construction, and tech support (I answered calls for 3 years).
This is also my experience being married to a nurse. Any story I have about a boss, coworker, or client being a jerk, she has about five stories about someone being bad enough that I'd already be shooting resumes toward anyone who will take me.
She's been punched in the face by a patient, she's had coworkers who sabotage each other due to personal vendettas, she's had bosses go on racist tirades in meetings, and on and on and on. As I remind my wife whenever she has a particularly awful day, there's a reason why the classic NP-hard CS problem is literally named the Nurse Scheduling Problem[1]. And yes, she's considering a career change.
Yes, my wife has also been punched working in the hospital. She now does nursing by phone where people are still really awful to her, but at least they can't assault her.
All customer-facing positions have to deal with rude customers. Very few of those positions specifically select for customers with a high correlation to selfish and/or antisocial conspiratorial behavior. Almost all COVID hospitalizations are unvaccinated, and there's a very large (if not majority) portion among that population that chose not to vaccinate for entirely selfish reasons, and another large portion who have been actively consuming media telling them the members of the medical profession are the enemy. You'd be hard pressed to select for a more adversarial customer base.
This isn't particularly reasonable analysis. A large chunk of the unvaccinated population is elderly and contraindicated for vaccination or in hospice care. From talking with nurses, the elderly population has its own set of problems and frustrations. Imagine trying to administer care to someone who has no idea why they're in a hospital setting. Similarly, vaccination status in American COVID-hospitalization research classifies people of unknown vaccination status as unvaccinated. These people are often homeless, isolated and elderly, or mentally unwell and unable to provide reliable information to caregivers. Again, likely unpleasant to work with.
Grouping these people as conspiratorial is unfair and seems politically motivated. While you definitely have some overlap with conspiratorial people, people have a right to be skeptical of medical care, which is often incorrect and potentially life threatening. Being able to explain things concisely and with evidence is a core skill for a nurse, much like being able to explain to someone why their technical decisions are setting them up for failure is a core skill for a software architect.
But from talking to nurses, this isn't the drive for negative workplace satisfaction. Patients who are hospitalized are less likely to be mentally stable: many pathways to hospitalization come from extremely poor decision making, and many of these people are repeatedly hospitalized. Combine this with the fact that it's a very physical job, primarily handled by women, and you have a multi-faceted problem that's not as easy to solve as just giving people right-think.
Personally I think the pathway to fixing this is appropriately valuing nursing care, what is often a highly-skilled profession with large physical, legal, and downstream risk, and compensating people appropriately. While nursing is a disproportionately paid job relative to educational requirements, current compensation really doesn't accurately account for just how demanding a job it is.
The amount of nurses you see who become addicted to painkillers, benzos, etc., is truly sad. Much like teaching, it's an area where I feel that society is inaccurately evaluating what the overall impact could be if the role functioned well.
Yeah I don’t know about that bud. Try telling the spouse of a dying person that their half baked ideas they read on Facebook aren’t valid and tell me their meltdowns are comparable to working retail.
All jobs suck donkey dick, but jobs directly dealing with sick and dying people are on a different level.
Most industries are neither tasked with restoring health nor with being the bearer of hard truths about a person's health. I think it stands to reason that healthcare can be a particularly toxic environment for those reasons.
Half of the toxic problem is from the people being treated. The other half (and sometimes more than half) is from management and co-workers (i.e. doctors). Not all doctors are bad but enough of them are to make an impact.
Absolutely. In case it wasn't clear: I was saying that just dealing with peoples' health makes for a fundamentally stressful and potentially toxic environment, even if each individual in question is perfectly kind and reasonable.
Mistreatment by doctors and management isn't excused by that, but I think it can be seen (partially) through that lens.
Health care seems to be part of the institutions that are of no use to certain cults. It's part of the effort to dismantle the administrative state and reserve health care for the 1%.
When I was young, in the 1950's. Nurses were respected, as were teachers and so on - we generally learned from and respected our elders. In the intervening period disrespect has grown, and chastisement has declined.
Respect and disrespect are still there - we have Lord of the Flies played out in our school yards daily. The strong and socially facile bully/beat and establish gang structures. When I was young = 95% white, and the weapons were fists. Now gangs are color coded and are better armed. Disrespect a person now = diss someone, and you either yield = be the toad = toady in the manner of toads.
Humans seem to need to be closely supervised to forestall this = Big $$ for watchers.
Our school was square with long halls with class rooms on each side, wide double run stairs, three floors. Every hall segment between stairs = 1 teacher. Every landing = teacher. Recess was boys and girls apart grades 1-8. Mixed above, but every yard area had 2 teachers.
Now these areas are ungoverned and the gang hierarchies rule the areas.
I think a computer guided system would help. My experience in lower grades, high school, college and grad school is that there is a consistent lack of showing students the concept of self-study, this is exemplified with the famous self studiers AKA autodidacts, like Newton as a prime example.
This skill is a very important one to develop early in children. Sort of give a person a fish a day - or teach him how to fish.
Online teaching at all levels up to and perhaps including grad school is well suited to complex programs that show a student a module of this or that.
This can be history or mechanics. After the module is presented, the student is queried on the facts of the lesson and then asked what he can deduce from the lesson.
Say the 300 against the Persians - why did the Persians fail? The student should then deduce that because the front of battle was only 30 people wide that it was a battle of 30 against 30, and better training, armor, skill and weapons that meant the Persian masses were useless - it was an attritive war of 30:30 until one side lost enough men that it became 30:29, 30:28....30:1 = war over.
Some students have greater intelligence and will analyze this aspect correctly. Those that do not are sent to the first fork..... and on to the full analysis.
In this case, the Greek better arms/skills may well have endured until the entire 300,000 Persians were killed, via re-supply from various Greek city-states - in this case, the Persians did an end run and were able to change the combat ratio to the point where the Greeks were overwhelmed.
Going to the general case:- The auto-didactic skill of the student needs to be developed one-on-one via the skillful design of the course material, with forks and subforks and re-entrant forks into the stream as each student masters an item and proceeds. At every point there should be a fork for every fail point - you can have as many forks as needed to imbue understanding. Modern computer systems are quite capable of this degree of complex interaction - but it requires a good amount of work with both masters in topics(many of them to variegate the forks) and up to now I have seen few produced. Large amounts of $$ and time have been spent on thousands of parallel minimalist approaches - it needs a central command/fund structure. /rant...
- High responsibility with unsafe conditions. You're literally responsible for people's lives. Poor staffing ratios stretch you thin and make you more likely to make mistakes. And if you make a mistake, you're at huge risk for litigation... and now criminal consequences too. Responsibilities, resources, and staffing stretched even thinner due to the pandemic.
- Administration that treats you as something to be optimized and does the absolute bare minimum to support you. Instead they tack on additional tasks, expectations, and requirements ("no water at a nurse's station!"). They encourage a culture where nurses provide a concierge service to 'guests' instead of critical care to patients.
- Hostile/entitled patients. I'd guess many/most patients are not an issue, but it only takes a couple of difficult/combative patients to really ruin your conditions.
- Low pay given the responsibility and working conditions for non-travel nurses. https://nurseslabs.com/nurse-salary/#nurse_salaries_by_state Like many others pointed out here, in tech I make way more than a nurse for a job that's less demanding, has far lower stakes, and is of far less value to society.
To me the blame lies mainly in middle/upper management, whose role is to build and empower an effective workforce. If 90% of your workers are considering leaving, you blew it.
The traveling nurse phenomenon is exemplary bureaucratic absurdity. To paraphrase a conversation with a nurse friend:
Nurse: It's really hard for us to hold on to our good nurses, we can't afford support staff so they get stressed out and leave for traveling gigs.
Me: Why can't you afford support staff?
Nurse: The traveling nurses cost 3x more. We have to hire traveling nurses to replace the ones that left for traveling gigs.
Me: ...
Nurse: I know...
Me: Can't we just... pretend they are all traveling nurses?
Nurse: I know...
I'm not a big fan of defrauding your employer, but sort of hope that some of these "traveling nurses" are somehow swapping gigs secretly and subletting their temporary housing to college students.
Part of it is that travelers are contractors. Management only has to pay for that contract for 3-6 months, then technically that cost is no longer an issue.
Whereas an FTE nurse is a recurring annual expense, so higher wages will lead to higher long-term costs.
Everyone in hospital administration is expecting demand to die down once COVID surges die down, so they don’t want to make any long-term financial changes.
Some of these conditions have always existed. But I can't imagine 90% have wanted to quit in the last decade. The most important factor thus is most likely COVID
Like with many jobs Covid revealed what society truly values and what not. Sure clapping for nurses, nice.
But these people should have propper working conditions and wages, otherwise nobody will want to do the job.
Covid just gave the realization that even if we face a global crisis where nurses are dying on the front, the rest of society is not willing to provide the bare minimum these people deserve.
Exactly this. The nursing profession has been accumulating empathetic debt for probably decades. By empathetic debt I mean nurses taking on more work and responsibility beyond personal rational choice because if they fall short then patients suffer.
the truly tragic part of all of this is that as much as we would like to imagine these nurses confidently walking away from a bad situation like some sort of power move.. a lot of them are not. A lot are finally leaving because they are broken and feel broken enough that they dont feel capable of being responsible for patients anymore.
To reiterate- many (most?) nurses that quit still want to help people, but no longer feel capable of helping. That is a level of trauma that can be passed down to the next generation. It might take effort to let the gravity of this reality sink in.
Anecdotally, my mom is a nurse and she has come home and cried due to sheer helplessness to her work problems on more than one occasion. Shes near retirement age and switched careers into this late in life to help people so this is pretty much it for her. If the system does not show mercy and continues to grind her out then she leaves the workforce feeling helpless and broken.
It goes beyond payment. better pay will go a LONG way, and is absolutely necessary.. but it is not enough. There needs to be more redundancy, because 100% utilization of that kind of resource in that kind of system is something that would get you a failing grade in system design.
I honestly have no clue how we fix this problem. Our healthcare costs are already out of control, COVID showed our systems can’t handle large numbers of patients, and we’re finally nearing the point where we get healthcare out there to all the people who need it.
Who’s going to care for all of them? Do we just make healthcare even more expensive, raise everyone’s pay, and hire a fuckload of new nurses? I’ve never heard of an RN being out of work for very long; I can’t imagine there’s a lot of well-trained RNs looking to be hired. Seems like we’ve backed ourselves into a corner we’re about to wall off.
Does anyone know how we fix this? I’m very interested in hearing ideas.
>I can’t imagine there’s a lot of well-trained RNs looking to be hired
I think this is an assumption we have to accept. The implication is that there are not enough nurses. Which means we need to protect the ones we have, and incentivize people to join. And we need to be creative / strategic / tactical about it because it is not a problem we can just throw money at (and as you mentioned, the money doesnt exist anyway).
Step 1: protecting the nurses we still have.
a) Increase denial of care. Nursing seems to be in need of triage. Or rather, "the system" needs to bear responsibility for triage instead of putting the weight on nurses and simply forgiving them for reasonable mistakes as a result of being overloaded
b) Reduced workload for nurses. Formalize the maximum acceptable workload for a nurse. Maybe provide compromised solutions that patients can agree to for any work beyond the maximum (less documentation, less liability, etc - an acceptance akin to treating a soldier on the battlefield. ie "do whatever you can, i'd rather something than nothing")
c) Increase usage of care workers (cheaper workers that RN's can delegate some responsibilities to)
d) Make a public awareness of how loaded a healthcare locations workforce is (so patients can self-manage in the moment; ie. my urgent care is very busy right now, let me go a couple towns over)
Step 2: Incentivize new nurses
a) Measure how many RN's exist that are not working as nurses. Do a case study to see what would bring them back
b) promote the profession to the youth like we did for STEM in the 2000's
c) reduce training needs. break apart the responsibilities of an RN and group them by categories that non-RN's / care workers can become certified in. allow RN's to delegate more work to "nursing category specialists" like IV management, medical history relevance, cleaning up shit, covid testing, etc. (whatever categories make sense)
Step 1 will support step 2, as it will be easier to recruit new nurses if nurses are better protected.
the important thing to remember is that we cannot control the demand on the healthcare system. We need to protect that system from collapsing if demand becomes too high. We must also provide a means for providing some treatment instead of no treatment in situations where full treatment is not possible due to excessive demand.
Personally, I think we coddle patients way too much. I understand wanting to protect people from their own stupidity, but we really need to stop trying to make the healthcare system a pleasant customer service experience. Let them be busy level-4 service technicians who do not have time for our bullshit.
Hire a much cheaper dedicated friendly person to provide friendly interaction. have them relay anything medically relevant if it pops up. Let them be the first person to show up to the room and decide if a nurse is really necessary, etc.
Basically, i think we need to evolve / progress RN's to be more like Doctors and prop up a less qualified class of healthcare worker underneath the RN's
> Low pay given the responsibility and working conditions
The pay to responsibility ratio for nurses is absurdly low. So unfortunate given the difficulty of the profession. I guess we'll see if anything changes over the next handful of years.
The pay was good enough last year, what changed? In my opinon nursing has always been a difficult job, yet they've always had people lining up to become nurses. So it must be more than just 'the job is too demanding'.
Pure speculation, but if I had to hazard a guess, it's because the job is becoming increasingly inhumane.
More and more, nurses have to act like robots to remain in compliance, and that's not what any of them signed up for, and the increasing lack of intangible reward that comes from caring for people and creating a human connection, means they demand more explicit monetary reward for temporarily suppressing their humanity to do the job.
I think most of what I listed, except pay, has gotten worse since the pandemic started.
- A large fraction of patients see the pandemic as overblown and nurses as perpetuating the myth. It's gotta be hard to care for someone who mistrusts you from the beginning.
- For those nurses taking care of COVID patients, it's probably tough to watch the cycle of death, and moreso when you know many could have taken steps to prevent it.
- The pandemic obviously puts a strain on the healthcare system, including its workers. More patients, longer hours, etc surely gets to be exhausting after doing it for 2 years.
- Administration that says they care but do the bare minimum to boost conditions or morale. A pizza party isn't as meaningful when you're struggling with an unsafe patient load.
- There's a feedback loop. As more nurses quit, the burden gets heavier on those who remain.
So even if pay hasn't dropped, the conditions have gotten worse. It's not a surprise that eventually people decide that it just isn't worth it anymore.
COVID protocols and protestors, combined with the decay of the ongoing K-12 and college education system, Great Resignation, and general economic malaise of Millennials and Zoomers.
I have a close relation that works for one of the oldest pediatric hospitals in the country. It was recently revealed that they will be shuttering almost all pediatric services in the next year because they can 10x their profits by only serving elderly clients. The entire purpose of this organization was to provide pediatric healthcare, and it wasn’t losing money…
Sometimes, it feels like we’re min-maxing ourselves to death over here.
The Invisible Hand works generally fine-ish for non-essential and commodity goods. People might be sad their favorite store went away, but, for the most part, life goes on. It seems to even be the least bad way to handle these sorts of things.
It's a bit harder for me to see this as an acceptable approach to health care. Not every segment of the economy needs to be a constant drunkard's walk in search of maximum profitability in the aggregate. Sometimes what the public actually desires is stability and reliability.
If there was a perfect way to attribute drawing people to an area, and how much they spent, I suspect some businesses would have rather different rents.
I had a friend who ran an unprofitable arcade for some time. His trash was nothing but food and drinks from other local businesses, particularly piles of bubble tea cups from a place across the street. It seemed rather likely it was worth paying him a bit to stay there.
Will people pay more for stability and reliability? If so, then that is what businesses will optimize for.
Businesses exist to give us what we want. Those that do it well are profitable, those that don’t aren’t.
Keep in mind that the effort spent to make healthcare more stable could have instead been used to provide more healthcare overall. Or something else entirely, like shoes or haircuts.
All services are not as good as they could be, because the effort beyond “good enough” gets shifted to some other more valuable purpose, where things are not good enough yet.
> Will people pay more for stability and reliability?
Given that the USA pays higher-than-average prices for poorer-than-average outcomes, I'd say this is a spurious hypothetical, mostly useful for helping to demarcate the point where economics ceases to be an empirical, scientific pursuit and instead becomes a sort of low-rigor offshoot of moral philosophy.
But, back in the realm of epiricism, we know that this is one of those situations where closer government regulation can produce higher quality of service at lower cost, because the rest of the developed world has figured out multiple successful formulae for doing so. The only clear downside, if you can call it that, is that their hospital administrators don't seem to have quite such large collections of luxury watches.
I think you are implying that most people are 'happy enough' with the current businesses they interact with.
Most people realize that a business will only change if a significant portion of buyers change their spending habits, and individually choosing to not support a business out of ethical concerns only hurts themselves.
Then there ends up being a lot of people who buy products from businesses they hate, and would support collective action against those businesses, like passing laws.
People like that aren't dumb, they are just trying to work around how their next best option is so much worse than buying the original product.
People are selfish, a dash of prisoner's dilemma, a pinch of tragedy of the commons, and you get businesses that serve individuals while failing society. Also efficiency is the enemy of robustness. No one wants to pay 10% more for slightly inferior hard drives, until a flood destroys the entire worlds production capacity. I consider myself a libertarianish sort of thinker, but market forces are a greedy algorithm, with all the downsides of that.
>> they can 10x their profits by only serving elderly clients.
> Soon people stopped coming
Ah, yes. Why didn't we think of this before? By increasing the cost of (geriatric) healthcare, we can destroy demand. That's how supply/demand curves work right? In this way the invisible hand delivers unto us a fountain of youth ;)
Old people in the USA are EXTREMELY wealthy in terms of healthcare purchasing power. All retired people have medicare. Many retired people have additional healthcare coverage from their former employers (doesn't exist anymore -- disappeared along with pensions -- but this benefit used to be common). Many retired people have significant savings in addition to medicare and private health insurance.
Most new parents have little to no government assistance, do not have significant expendable income, and have little to no accumulated wealth. Children, of course, are even poorer than their deadbeat parents.
What I was told is that elderly people need more and more frequent care. Additionally, reimbursements tend to be higher for the procedures elderly people need vs children.
No, more likely you'd see a ton of alternative medicine and self-diagnostic/treatment options for young people. I'm not entirely sure that I wouldn't want this.
Yeah, young people rubbing tea tree oil on their tumors, drinking spoonfuls of olive oil to cure their appendicitis, and vaporizing fruit peel oils to “cure” kids of infectious diseases. Just what the world needs more of.
The first, mentioned already in this thread, is that maximizing profits should not be the ultimate yardstick in all cases.
The second is that we are not setting incentives correctly in healthcare: preventative care still plays second fiddle to curative care. If the healthcare industry were purely free market, this could be attributed to individuals not understanding the long-term benefits of preventative care, or overly discounting the distant future. But the healthcare system is not purely free market. The largest payers, public and private, could do a lot to correct the incentives by setting their reimbursements accordingly.
Becoming a hedge fund is actually a bad idea if you are only after profits because it is unclear that over long-time horizon this is actually a very profitable activity. We only remember the winners.
So, a hospital can close a service with no repercussions, and if workers at a "critical" secure decide to strike they'd be ordered by a judge to get back to work...
We’re facing some massive generational crises at this point, and it feels like the only solution is to wait for the current leadership to die off, and hope the gen x’ers fix it.
The WWII generation fixed the ozone hole, but their kids didn’t lift a finger for global warming.
Subsequent generations are scrambling to pick up the pieces for our kids, while crap like this, and our rapidly collapsing democracy keep sabotaging our efforts. Heck, in California, we’re actively causing psychological harm to an entire generation of kids (with masks) because of a tiny minority of anti-vaxxer school teachers.
Of course, progressive boomers exist, as do idiotic younger people. However, the current generation of leadership in the US has completely failed us.
Anyway, it’s not surprising to me that that crowd decided to shunt healthcare resources away from their (great) grandkids and into elder care.
I'm increasingly thinking politicians should not be allowed to make decisions that won't impact them. We've got people that will be dead in 20 years preventing action on global warming.
They won't live long enough to have to deal with their consequences of their actions, and they clearly don't care if they burn the planet down before their kids inherit it.
I think this translates to an age limit of 65-75.
More importantly, I think this should be applied to voters as well.
Please, don’t spread ageism. Yes, brains perform worse in many kinds of ways when they age. But that’s highly variable. And there are narcissists and sociopaths in every age group.
The kinds of ways matter. A primary way the majority of brains start to show age is in trust and risk assessment. [1] [2]
I agree, someone with a compromised ability to evaluate risk is probably more than capable at doing most desk jobs. However, the last thing we need is politicians who's aging brains have been compromised in evaluating future risks. Putting someone most likely to send scammers gift cards in charge of foreign policy and assessing climate change risks is simply a recipe for disaster.
It doesn't seem all that crazy to demand that the ~300 people running the US not be at an age where mental decline is common.
High testosterone correlates with aggression, and young people have way higher T than elderly. Should we ban people in the highest T quartile from becoming politicians? Of course not. It's a complex and highly individual problem which can't be solved by filtering via just one variable, like age, gender, level of brain deterioration, or some hormonal level.
Here are some problems that _don't_ prevent people of any age from becoming a congressman or woman:
- Alcohol abuse
- Narcissism and/or sociopathy
- High debt
- Cult membership
- Most importantly: Personal financial interest in specific policy changes
Why not start with these? Banning elderly because they on average tend to be more gullible seems like a weird way of addressing governmental issues.
On a different level, I find the idea of banning people from governmental positions based on a specific trait deeply undemocratic, and a slippery slope. Principiis obsta.
> We’re facing some massive generational crises at this point, and it feels like the only solution is to wait for the current leadership to die off, and hope the gen x’ers fix it.
oh man, I choose to laugh so I don't start crying hahaha.
I want to turn this into an argument of why age-reversal and other longevity research is such a bad idea (personally, I think it's kind of evil; but maybe I've seen too many villanous cartoon characters throwing everything under the bus so the can live forever).
I mean, making sure Putin doesn't live forever seems like a pretty high priority to me.
There's also the fact that science might lock up, since old scientists have more reputation at stake in the old theories (there's an adage "science advances one funeral at a time"). We're not ready as a species for immortality
When people say stuff like this, are they being hyperbolic or do they actually mean it? How long is the democratic tradition in the US that is collapsing?
We just had a candidate openly try to steal the last presidential election and face no real consequences as a result. In fact, it likely strengthened his position. 10 years ago I would have thought the end of American democracy was extremely unlikely, now though we're only a few small steps away and that bridge could be crossed at any point.
This isn't some outlier event either, democracy has been receding around the world for years. I really, really hope the trend reverses itself, but am scared at how real the threat is.
I don't think we were even remotely close to somehow Trump remaining on as president.
> democracy has been receding around the world for years
I am skeptical. Majoritarian democracy in the US has only really existed for 40-50 years and I perceive it as continuing to expand both here and abroad.
That’s pretty naive to think Trump wasn’t even close to remaining on.
If enough states had sent contested election results (eg a county or state’s election board is tied in approval or does not approve the results because of one die-hard) then the matter would have gone to the house of reps.
How many of those reps voted not to certify the election results? Now, in the event of contested state results, each state in the house of reps would get one vote. There’s more red states than blue states…how many unscrupulous representatives, who already voted not to certify the results, would it have taken to grant Trump the election?
For what it’s worth, many of the key states in the election had narrowly certified election results. In some cases it came down to a single individual who could have flipped the other way, and the results would have been contested.
You do not realize what a narrow path democracy treads. The anti-democratic forces do understand this, and the last few years have been empowering to them.
And that’s an easy scenario that doesn’t even take into account the very real possibility of political violence - don’t forget that people showed up to the US capitol with weapons and tools for kidnapping.
Honestly I find your take to be either naivety, denial, or willfully obscuring the truth to promote anti-democratic goals.
It's possible we have too much democracy. A lot of stuff got changed because we thought the previous configuration didn't make sense but it may have been that way for a reason.
Referenda that can't be overriden by legislature should require 50% of eligible voter population to support, not 50% of voters in that particular election.
It would need to apply to everyone. No more of this open up single family housing is this middle class area while protecting the parks / forest in the wealthy areas.
What about things like AirBnB? Limiting those is a form of NIMBYism as is limiting where factories and polluting buildings can be placed and/ran.
> Why register as a not-for-profit when you’re profitable?
If your purpose isn't to return a profit to stakeholders, but to serve some social purpose eligible for charity nonprofit status plus like “pediatric healthcare”, registering as a nonprofit gives you more surplus revenue because of tax exemption and the ability to accept donations that are tax deductible for the donors.
nothing about being not-for-profit means you can't make a profit. it just means you don't return those earnings to the shareholders and thus find yourself governed by those shareholders.
There's no such thing as a "free market" for healthcare. The ability for consumers to exit a market is one of the prerequisites for the invisible hand effect. You can't exit the healthcare market.
I think you're being purposefully obtuse, but here's why:
- SNAP / EBT / Foodstamps for people making so little money. Add onto that, Food banks.
- Farm subsidies for many cheap foodstuffs (Corn) causing massive cheap, albeit junk food that can sustain.
- I can literally grow food in the ground for "free", put it in mason jars and save my food for a year. I can't open a fresh can of broken-arm at the fixed cost.
- Food is fungible, if I'm hungry, I can wait 2, 3, 8+ hours to eat, or have a quick snack until meal time. It's not like I need a Big Mac infusion in the next 10 seconds or else I'll die from lack of special sauce.
- You have many options of food. You can eat Soylent, rice&beans, or steak for every meal at various price points. You don't really get an ala carte when it comes to Chemotherapy.
At least here in the Midwest, people grow food all the time. Can’t grow strawberries in December, of course - but we eat up canned goods from friends/family throughout the winter.
This is a bad faith question asked without any basic thought.
Within 5 miles, I have at least 10 different grocery stores to shop at. Each will carry hundreds of products at less than $10 each. Not only do I have tons of choices, but the pricing is completely transparent. And that's just grocery stores. Add restaurants (Both sit-down restaurants and fast food), and that number quickly reaches over 100 within a 5-mile radius.
If I'm in a medical emergency and someone dials 911, I'm likely just being brought to the nearest hospital. I have zero choice in the matter, and will come out with whatever bill they want to charge me.
Even in non-emergencies, good luck shopping on price. Doctor offices don't like giving that out.
There's competition in the food market, but not healthcare.
> This is a bad faith question asked without any basic thought.
Where ad hominem is a hallmark of good faith discussion.
> Within 5 miles, I have at least 10 different grocery stores to shop at. Each will carry hundreds of products at less than $10 each. Not only do I have tons of choices, but the pricing is completely transparent. And that's just grocery stores. Add restaurants (Both sit-down restaurants and fast food), and that number quickly reaches over 100 within a 5-mile radius.
This makes sense if you're aware of the fact that each human being eats three meals per day.
> If I'm in a medical emergency and someone dials 911, I'm likely just being brought to the nearest hospital. I have zero choice in the matter, and will come out with whatever bill they want to charge me. Even in non-emergencies, good luck shopping on price. Doctor offices don't like giving that out.
I clearly conceded the point that you can't exit the healthcare market.
> There's competition in the food market, but not healthcare.
Are you under the impression that I disagree with this statement? Consider reading (and, ideally, understanding) the thread in which you are participating prior to commenting.
Food, shelter and clothing generally have discoverable pricing.
I challenge you to find the price of a cancer treatment regime protocol in the United States. I will bet you any amount of money you care to wager that no US provider exists anywhere that will give you a price quote for lung cancer treatment in writing anytime before that treatment is provided.
And even IF you could, that only covers the cases where you are still have enough health and mind to rationally evaluate the prices. If you've been in a car accident and are dragged unconscious and bleeding into the ER, you can't shop around, even if they DID give you a price, which they certainly won't until you're already treated.
I agree with your points, but I think there are narrower solutions. With respect to pricing, the problem seems to be the negotiations between hospitals and insurers, as well as hospitals' failures to institute cost-accounting. Forcing them to do better accounting, and have a clear price-list would probably help, but getting rid of the employer healthcare tax subsidy (or expanding it) would likely be a better solution.
With respect to ER care, it does seem impossible to 'shop around', but these cases make up a minority of healthcare expenditures. Perhaps government should cover these cases (though this could have horrible incentive problems), or this type of insurance should be separated from the rest, and somehow priced clearly and in advance (according to level of care) by a cartel arrangement or state regulated rates.
> though this could have horrible incentive problems
I hear this argument, but I don't buy it. What's the incentive exactly?
That people will hurt themselves, so they can go to the ER for free? That's nonsense. Nobody wants to get hurt, nobody wants to get sick, getting hurt or getting sick is not a good. The fact that they don't have to pay to "get hurt" isn't an incentive. Perhaps a few people feel this way and are insane, but those people probably need to get help at government expense either way, before the government ends up paying for them to be in prison or institutionalized anyway.
> Forcing them to do better accounting, and have a clear price-list would probably help, but getting rid of the employer healthcare tax subsidy (or expanding it) would likely be a better solution.
Believe it or not, it would be way easier politically to implement Medicare For All than to do piecemeal reforms.
'Medicare for all' will cause a number of foreseeable and unforeseeable problems (and benefits). It would be interesting to see one or more states do it, and observe the results.
How can a state do universal single payer of its own design when there are multiple direct federal health care systems covering a substantial portion of the population, plus a huge tranch of the money states rely on for health care tied to a federal/state cooperative program with federal programmatic and eligibility constraints?
I think the experience in Vermont suggests that it's unlikely to ever happen at the state level. It's far more likely to be a big bang at the national level.
Sure you can. You can decide that you are not going to enrich an industry that basically does nothing for you in the long run. Everyone ends up dead, and I for one do not plan to spend my final years under constant care from a industry that is designed to drain every last dollar I have before I pass on.
I think the majority of people say something to that effect at some point in their life. But the only real alternative is suicide of some kind, and how many people actually follow through with suicide?
Actually, that’s exactly how unfettered “free market” capitalism operates. The end game is big companies end up controlling everything, including the regulations in order to tip the scales in their favor.
The healthcare industry disaster wasn't born out of regulatory control - though money does now follow the regulations. The disaster was born out of regulatory mistakes(in particular, look back to the 1940's when the govt made it tax free to offer health insurance as a benefit). [1]
The industry is an onion and in order to understand why it is the way it is today you need to peel back all of the layers that have been added by the govt over time and the unintended consequences of those.
Wait, wait, wait--you're saying that we need to solve issues like regulatory capture through legislation... so that we can have a market without governmental interference (aka a "free market")? Huh?
You can't on the one hand tout the "free market", while on the other complain that we don't have the "right" kind of governmental interference.
Even if you could square that circle, it still sounds disingenuous to argue that we could have the most efficient system if only we were to eliminate _thing that said system actively encourages_. The failure is baked into the game, my friend.
I don’t think that reasoning is necessarily unsound. For there to be regulatory capture, there needs to be regulation. The legislation proposed could be to remove or minimize that regulation, and thus limit the ”hooks” whereby to capture it with. Replacing ”governmental interference” with ”less governmental interference”, not ”different governmental interference”.
I don’t take such a libertarian view myself, by the way. Just pointing out that I don’t think you can pick apart the argument of the person you replied to in that way.
Instead of advocating for and gambling on a "free market" health care system that has never been tried successfully anywhere, and hoping that it will work out (because dogma?), why not advocate for systems that have been tried all over the world that have been proven to work?
I'd sign up for a significant increase in my taxes if the US system were replaced by the system that I experienced in Belgium for the first 30 years of my life.
And by successfully, I mean: everybody, irrespective of income or status, can expect to get the care they need.
The free market healthcare system in the USA worked great up until regulations pushing out mutual aid societies completely changed it. Costs were affordable for everyone.
It takes an exceptional breed of ignorance to say "just implement whatever <country> has" as if that is a silver bullet and that the same forces that caused the current debacle wouldn't also do their magic on anything we attempt to transition to.
If it was as easy as paying out way out of the problem we'd have done it already.
It also takes an exceptional amount of knee jerk assery to interpret my comment as "change the US system to the Belgian one". The Belgian system is one that works more or less from my experience. Most inhabitants of Germany, France, the Netherlands, and others will claim the same for theirs.
Nobody is claiming that the US should copy the system of some specific country verbatim. But it's equally dumb to dismiss the common traits of these other systems, and say "nah, let's do just the opposite."
>It also takes an exceptional amount of knee jerk assery to interpret my comment as "change the US system to the Belgian one"
Well you literally said "I'd sign up for a significant increase in my taxes if the US system were replaced by the system that I experienced in Belgium for the first 30 years of my life" so why don't you tell me how that was supposed to be interpreted?
America shares a very long border with a nation with a functional healthcare system and we generally prefer to compare to them.
I wrote "why not advocate for systems". Notice the plural form. Did you assume that by writing "all over the world", I actually meant the superpower of Belgium?
What all those systems have in common is that they are a mix of free market and strong regulation. The opposite of "let's do even more free market than what we have now."
I don't know how the US can get there. It's probably impossible, just like school shootings and the "No Way To Prevent This,' Says Only Nation Where This Regularly Happens" argument.
Feels a lot like 'Real free markets have never been tried!' which we all know from its standard form on the left. If, at this point in history, real free markets have been unable to sustain themselves in the areas of the economy that people depend on the most (healthcare as a major example) then perhaps we ought to consider whether they're able to sustain themselves at all. I believe free markets and meritocracy are two systems commonly pointed to today that may be 'ideal' in one sense or another but which in practice cannot help but sow the seeds of their own destruction.
Markets exist by virtue of laws created by governments - property law being the primary example - expecting actors in a free market who aggregate enough wealth to affect those governments not to just strikes me as unrealistic. It reminds me a bit of gaming. Everyone agrees that in a competitive game the most fun part is early on before a 'meta' can be established. But of course that meta will always end up established and it's basically dumb to be mad at people for metagaming or to otherwise expect them not to.
> Free markets are the most efficient way for information to be transferred throughout the system.
What do you think of VC-funded "growth" companies that lose money for years while providing products/services at below cost? Is this a case of the free market working or of it being subverted?
There is no such thing as free market capitalism. This is why the parent comment said "capitalism" and not "free markets". I assume that's what you meant by putting "free market" in quotes, I'm just making an explicit clarification.
I would say the drug cartels are about as close to free market capitalism as we have today. They are largely unregulated because they can either buy off the regulators / government, or fight them with armies.
> I don't think the US can be summed up with a single word.
I think it can, I've been thinking about this and it's "scam".
Like, think how often everything in our country is a straight up scam. Healthcare, parking tickets, basically anything you buy. It's almost all snake-oil flim-flam every which way and as a 'consumer' you have to wade through the mire every single day to get scammed as little as possible.
So true! Everywhere I turn it's just people trying to extract the maximum amount of money from me for the minimum amount of value in return. It can't be good for our psyche.
I don't even think Marx would agree with that. He thought capitalism produced a stage of history that wasn't exactly capitalist, which then would inevitably produce communism through socialism.
He could have and did: factories and craftspeople from Adam Smith's world are the epitypes of capitalist activity. Giant corporations that half-merge with the government are Marx's final, dying and barely capitalist stage of capitalism, that hardly involves markets at all. He thought capitalism (factories and craftspeople) would reach the end of its lifespan and give birth to $THC or $HCA.
Sure, but that's like blaming "humanity" for all the woes of the health care system. It's humans who produced the health care system in the US after all.
You have to be more precise as there are clearly aspects of capitalism that have resulted in tremendous improvements in quality of life (look at North Korea vs. South Korea).
Regulatory capture is one of the issues & revolving door politics. Especially a big problem in the healthcare & finance industries (the current head of the SEC spent his career at Goldman Sachs for ex.)
>Medicare ... will give them a blank check with tax payer money?
Whoever gave you that idea, you should stop listening to them.
Medicare payments are subject to a medicare fee schedule, which is typically much lower than a traditional private enterprise's fee schedule. What that means is medicare gets billed a lot less than a regular patient with insurance.
"Private insurers paid nearly double Medicare rates for all hospital services (199% of Medicare rates, on average), ranging from 141% to 259% of Medicare rates across the reviewed studies."
"The difference between private and Medicare rates was greater for outpatient than inpatient hospital services, which averaged 264% and 189% of Medicare rates overall, respectively."
"For physician services, private insurance paid 143% of Medicare rates, on average, ranging from 118% to 179% of Medicare rates across studies."
Medicare is not a blank check. It's a standard check (see sibling comment on fee schedules), and each check tends to actually be quite low of an amount.
The magnitude of "standard" and "low" are both demonstrated by the fact that when private insurers negotiate pricing contracts (basically, a one-off fee schedule) with hospital groups, they express prices in terms of "medicare multiples".
For example, the insurer will pay up to 13x of what Medicare pays for an fMRI administered under non-emergent circumstances with medically-justifiable cause. Pretty much every multiple is >1x, many are far more than 10x.
And medicare is arguably more expensive to provide, since the probability of confounding issues from disability or age is higher than in the general insured population.
Medicare is very consistent with paying, especially in comparison to private insurance, but the a la carte fees are quite "low" by relatively-freer-market definitions (I say relatively, because the reality is that private insurers negotiating with hospital groups is the antithesis of a free market, in most conceivable dimensions).
---
The main reason medical groups lobby against "medicare for all" is that they will lose lucrative "20xM" payouts from private insurers, and it's difficult to see how their ballooning administrative costs can survive on such a lean diet.
Of course, this line of thinking is deliberately ignorant of the thought that medicare fee schedules can be renegotiated to reflect the population of patients "medicare for all" would incorporate. But nobody's interested in thinking two turns ahead, let alone advancing the game state, when their pockets are nicely-lined on turn zero.
Another way to look at that is that Medicare is vastly underpaying for services, as the system is currently run. Basically, private insurers subsidize Medicare/Medicaid, and many providers either refuse to accept Medicare (as allowed by laws) or would go out of business without a sufficient private insurer base.
So, private insurers aren't charities that aim to support 'lucrative' payouts either. The often-huge gulf between MC and private (as you said) means that costs would have to drop massively if we did MC4A. Who's going to tell hospitals/admins, and more importantly, doctors and nurses that they have to take a 30%+ paycut?
The difficulty is that "cost" has a layer of abstraction that you may not be considering.
There are three acts in care. Act 1, you receive treatment and the hospital pays the nurses, doctors, and capital equipment. Act 2, the admin submits a claim and receives a quote from the insurer. Act 3, the insurer pays the admin.
One of the reasons why a certain treatment plan is negotiated at 20x Medicare is that, 50% of the time, the private insurer rejects the claim (correctly or incorrectly), and the hospital group needs to maintain payroll for an admin whose entire job is to contest the rejection and win the ultimately agreed-upon rate.
As you might guess, a large but difficult-to-quantify proportion of the quoted cost is this song and dance in Act 2. In Medicare, the distribution of Act 2's length is more predictable and smaller.
Nobody addresses this elephant in the room, because it makes private insurers and hospital groups look bad, but it's where a lot of ballooning "costs" can be explained away.
It depends on what you mean by "making money", but yes.
Basically, the "expected value" of a private insurance payout is usually not too different from the "expected value" of a medicare payout.
The sticker price of a private insurance payout is very high. The accounting department of providers love the sticker price, because they can carry them forward as payable liabilities, but a large proportion of private insurer payouts and patient deductibles are never realized. Stark contrast to medicare.
It's not because Medicare offers a "blank check"; after all--the amount of revenue that the hospital can generate will always be hard-capped by the number of beds+/physicians+/resources available.
They go with Medicare because the pay-out rate (i.e. "collect-ability") for billable services is much higher--and much more predictable--than if they attempted to collect/negotiate with non-governmental providers. A LOT of money is lost by hospital systems due to unpaid patient responsibility (e.g. insurance deductibles), which they can minimize by offering only services already guaranteed to be covered by Medicare.
My experience: I'm an icu nurse in the sf bay area. I make a good salary. However, you can make this and more with a job with less physical and emotional stress/abuse. Even the "best" hospitals like kaiser/stanford/ucsf are always short staffed. I considered another area of nursing/hc but it's really all the same BS of being short staffed, constantly being denied vacations, etc.
I feel like a waitress, custodian, social worker, therapist, punching bag and other stuff - It's never ending. This has effected my mental health so much that I am slowly doing my career switch to SWE. While I know every job has it's own difficulties bs/stress/politics, the one's i deal with as a nurse now I can no longer deal with. I don't regret this career path because it has taught me a lot, and their is something better for me out there.
Career: I did consider other areas of nursing, but they didn't satisfy me, ICU is relatively the most enjoyable for me. On a regular hospital floor/intermediate floor, a nurse will be given 4-5 patients and let me tell you its a ZOO! In ICU i only have 2, and those keep you busy the whole shift. They're both different kinds of crazy.
I will say, being a nurse in California is 5x better than anywhere else simply because their are laws that allow us to have uninterrupted breaks!
Happy to hear that you’re progressing towards a career path that sounds like it will be more fulfilling/better conditions.
I just wanted to say that it’s a sad state of affairs when we’re happy to expect uninterrupted breaks. Goes to show just how much we _really_ supported our frontline workers.
It rather reminds me of a zinger I read in an article about the plight of people trying to find good jobs after leaving the US military, written at the height of support for the War on Terrorism and consequent fashion for publicly, vocally "saluting our men (sic) in uniform":
The American people will do anything for their veterans except take them seriously.
On the plus side, if you are successful switching to software development, having a background as a practicing nurse will allow you to pretty much write your own paycheck if you’re willing to work in medical software.
Using an anecdotal source - My Wife (ICU RN) this is sounds right.
Outside of the existing issues with Bedside nursing (long days, physically demanding) - the primary issue is staffing. Pre-pandemic the ratios were already bad but now many are leaving for travel contracts which carry significantly better wages. It quickly becomes a loop where employees leave for Travel Contracts, and then can only be backfilled with Travel Contracts. The remaining FT staff nurses are left making much less money, and have to assist "training" with the outside Travel nurses. And while this is nothing against them - The travel RNs also often have a different "vibe" as they are much less focused on long term improvement or problem solving within the Unit.
Also ICU/PCU/ER nursing throughout the pandemic was a terribly depressing place to be. Leaving many of my Wifes colleagues (including herself) with what is essentially PTSD with little or no support from the Hospital System.
Should it? The market for medical care has a base rate (and appears to be clearly under-staffed for that rate), but (especially in a pandemic) it's rather peaky and the basic skills appear to be VERY transferable from location to location. If there are people with the skills that are willing to travel, it seems that a system that maintained maximum capacity in all locations would be a very wasteful one.
Yes, it should be indicative of a problem. The fact that nurses are overworked, and underpaid is a big issue.
> If there are people with the skills that are willing to travel, it seems that a system that maintained maximum capacity in all locations would be a very wasteful one.
The general idea here is that more and more nurses are willing to do this because they are underpaid and overworked in their regular (non-Travel Nurse) positions. I didn’t see anyone arguing for “maximum capacity” either… just better wages and working conditions.
> basic skills appear to be VERY transferable from location to location
If you read the parent comment by sllewe you will see that there are other costs and concerns around this which do more to stress existing nurses at whatever hospital is being filled with travel nurses. Imagine training a new someone every week (or however often new travel nurses pop up) while also having to do your own job… especially when you are already being overworked and when a miscalculation on your part could result in loss of life. All the while knowing that the travel nurse is making significantly more money than you, negotiated their hours of availability and doesn’t have to care about the unit beyond whatever contract length they signed up for..
I was referring to utilization level of workers, not stress or danger. If resources are planned too tightly, slight alterations can cause disruptions, so you might need additional workers.
I'd like to know what "considering leaving" means in this study. I consider leaving my profession every time a React hook misbehaves and locks up my browser, but I'm not actually going to leave. 90% seems way too high to be people who are actively wanting to leave.
> 90% seems way too high to be people who are actively wanting to leave
We are talking about the people who clean up the nastiest human waste that our bodies are capable of producing. I was already surprised that this number was ever less than 100% tbh
Yes, but that is what they signed up for - i.e. they knew it going in, and that has not all of a sudden changed.
I couldn't do it, and god bless them, but that is unlikely a cause of people leaving the profession - that would be like a computer programmer saying they were leaving the profession because they suddenly found out they have to stare at a screen most of the day.
I also find that '90%' number suspect as someone that works very closely with the healthcare community - there is a lot of turnover, and its hard to hire nurses right now - but almost always when someone leaves their job it is because they went down the street and got a 25% raise, i.e. they didn't leave their profession, just their job.
right, and while nurses do have to do some things I would consider gross, more often than not, it is the lower paid medical assistants and CNA's that get the real awful jobs that does not require a nursing degree - i.e. changing diapers in nursing home, bathing people etc - won't find too many nurses doing that in the nursing homes around me.
FWIW, comparing a misbehaving react hook with the challenges of being a nurse today feels weirdly entitled. Get closer to the reality of their job and you might start to understand why 90% want to leave (90% is a conservative number IMO).
If you’d cut your pay down to 25% of what you make, work 12h a day with a single 30min lunch break (that gets interrupted regularly), including several weekends and nights every month, without guaranteed vacations for holiday season/new year’s eve, work in a team that’s 50% understaff but still needs to deliver no matter what, without any carrer path forward, you’d leave your current SWE job right away. And in comparison, you’d still not be be even to close to what they do (i.e: cleaning up body fluids).
I thought it was pretty clear that I was joking about that part. My point is everyone has struggles with their job and may think about leaving sometimes.
For me, the question "have you considered leaving your career in the past year?" Is not specific enough to have a reasonable answer, so I'd like to know what the questions were more specifically.
Exactly, without any context this number is meaningless. How many were considering leaving a year ago, 3 years ago? We have no idea if this is a trend or even outside the norm -- perhaps nurses simply often run into days that make them reconsider their career choice.
Not surprising. My partner is a DNP and has pretty strongly considered leaving the entire profession.
From my perspective, the entire healthcare industry is set up to treat any frontline worker without an MD after their name as completely expendable, nothing more than a row in a spreadsheet that can be optimized for middle management to hit next quarter's bonus targets.
You can meet all metrics management sets out for you, have amazing patient satisfaction scores, etc, and every 6 months some spreadsheet wielding online MBA graduate is going to show up to turn the screws and tell you you need to work harder for the same pay, and to just be happy you aren't getting laid off.
At some point in time, the workers realize the joke is on them and find another profession.
This is totally anecdotal, so take it for what it's worth, but in addition to nurses leaving the profession I've seen quite a few doctors in my area leaving the profession as well. Relatively young men and women retiring the profession completely post pandemic, though I haven't had an opportunity, nor would I, to ask them why they left the position. I have no idea if it has anything to do with the pandemic or the administration or working with insurance =/
And one of these articles (the last) is from 2013, talking about a change in healthcare practices (corporate unification), the ACA (limits on accepting medicare patients) and the health reform law (liability reform). So, I guess medical burnout has been coming log before Covid and we have just been ignoring it?
I have no doubt that MDs are leaving as well - but, at least from my perspective, in any large healthcare system, there is a drastic difference between the way middle management treats MDs and the way they treat everyone else. The latter is completely expendable, whereas the MDs do have a fair amount of negotiating leverage around their working conditions.
I'm just sharing what I've seen - middle management treats MDs drastically different than NPs and PAs, even in states where the latter have almost the same scope of practice.
This is not to say that MDs don't have their own reasons to be mad at the system - insurance, changes in patient attitudes, etc.
I was at my family's Easter lunch last week and one of my uncles who's an MD was telling me about the mass exodus of doctors from the profession since COVID hit. Anyone who was thinking about retiring did so once the pandemic took off.
He then tried to convince me that I'm not too old to go to medical school. Yeah, no thanks.
Same story from my partner who is a PA. The private practice she worked for for years got acquired by a big name system and over the next 2 years they “optimized” a job she loved so far that she had to leave.
By the end she was seeing twice as many patients a day as before with no time to do admin stuff at work even after skipping her lunch break so she also had to do more work when she got home. The reward for doing double the work as before? A 10% pay increase barely above inflation. Meanwhile a few coworkers left and no new ones were hired so the workload just kept increasing.
It puts providers in such a bad position because the only way to push back is to drop the level of care, which has real human consequences.
Yes. Massachusetts which is NOT a right-to-work state. That means the union can negotiate a clause in the contract that any nurses working at the hospital must join the union. Here is a current contract that includes pay ranges:
A couple changes I've heard from nurses would be helpful:
1. Safe mandated staffing ratios. California is one that does this and many nurses seem happy with the ratios.
2. Safe harbor laws. If the nurse feels they are pushed into a risky situation, they should have a right to notify management which will take on liability if they do not resolve it. A few states have this but hospitals bully nurses not to invoking it.
3. Better pay for the liability they take. Unlike management, they could go to prison for mistakes they make. There was a recent case nurses were outraged about.
4. Unions are beneficial. In California the nurses union is pretty strong to negotiate better terms and conditions.
WHY THE NURSING SHORTAGE PERSISTS.
HALE T. N Engl J Med. 1964 May 21;270:1092-7. doi: 10.1056/NEJM196405212702105. PMID: 14121489 No abstract available.
STUDENTS' DISAPPOINTMENTS IN PUBLIC HEALTH NURSING.
HANSEN AC, THOMAS DB. Nurs Outlook. 1965 May;13:68-72. PMID: 14291737 No abstract available.
A good path to explore, but requires more data points than two from 60 years ago... Let's try this approach:
[0] steady with huge uptick since the pandemic
[1] steady decline with uptick in July 2021
[2] sparse, but slow incline since July 2021
[3] shallow dip ~2013, slow include since
Not to be mean, but 'leave nursing' and then what ?
Nursing is a well paying middle-class job without a lot of transferable skills to other professions.
Don't say programming. It isn't the solution to everything. Other low-entry-barrier jobs pay much less and have exploitation problems of their own. For a lot of middle class families, dual income is essential to maintain their lifestyle. So SAHM is not an option. Nursing has clearly gone through a rough 2 years, but I suspect that things are going back to normal now. Why leave now ?
> High patient-to-nurse staffing ratios
This bit is confusing me. If supply-demand is in the Nurse's favor, then don't they get more leverage on what QOL and wages they can demand ? It is not like they can fire a senior nurse on low pay, when new nurses are harder to find and demand higher wages. I know that the nurses refusing work and resulting deaths has bad optics, but it doesn't look like hospitals have a lot of leverage right now.
> Administrative burden and manual tasks
Sounds like an opportunity for a startup to disrupt the space. But, the jaded side of me thinks that the startup will fail due to insufficient political leverage with hospitals/insurance/law-makers.
> health IT
Keep calling it health IT and the problems will never be solved. Solving hard problems needs reframing of the resources dedicated to it. When tech workers are seen as assets and not cost-centers, these problems will solve themselves.
"If supply-demand is in the Nurse's favor, then don't they get more leverage on what QOL and wages they can demand?"
I have a family member who works in public health and is trying to staff nursing positions. She has something like a $400k budget to hire 4 nurses at $100k each (let's say). She is unable to fill the positions because cost of living in her area has gone up so much. She'd rather have 2 nurses at $200k each instead of zero nurses, but she's simply not allowed to do that. She's trying to change policy but it's a massive uphill battle.
Power's concentrated very high up in health care, and it's exercised through the use of rigid policies. It certainly seems like nurses should command higher wages, but the bureaucracy has become very effective at preventing basically anything from changing quickly.
When we got married, my wife (Physicians Assistant) made handily more than I did. $140k to my $82k midwest, software development job.
10 years later, she makes $130k (after cutting hours back) and I make $4-500k as a software engineer in the midwest. The two markets crossed drastically
$500K as a software engineer? That's the very tip of the unicorn's horn. My friend works as a CEO of a (smallish) software company and makes half that.
This forum almost certainly skews heavily towards people in Silicon Valley or working at Bay Area companies. AKA the very highest earning people in tech.
It's the difference in working at a public company that offers RSUs and bonuses vs working for a startup. Your base salary will be somewhat similar, but startups can't compete on total compensation.
It is a fairly common problem. We extrapolate our perceptions of the world from our peer groups. I had to suppress my urge for saying I am underpaid at $200k, because my non-tech (still STEM) MIT & Harvard grad-student room-mates would get annoyed at me. That's how messed up our circles can get, when STEM grad students MIT and Harvard are the poor ones. We live within many nested bubbles.
$250k still puts you in the top 2 Percentile of the US. So, while double the nurses would get to retire cuz of rich husbands, 98% would still be in the same pickle.
I feel like either you might be massively out of touch or this is a most not-so-subtle totally unverifiable flex ever.
I'm reminded of that episode of Arrested Development.
"I mean it's just one banana Michael, how much could it possibly cost? $10?"
"You've never actually set foot inside of a grocery store before, have you?"
Only in a vaccuum. It pays far worse than other jobs at the same rate given the effort and stress the job entails.
> don't they get more leverage on what QOL and wages they can demand ?
Sure, but it needs to get far worse. The hospitals are only going to budge once walkouts are organized. But that can't happen without strong unions, most nurses just need to pay the bills which is why they continue to put up with it.
I'm not sure you understand who has the leverage. The hospitals can let healthcare deteriorate far beyond current expectations. They still get paid in the end. The environment for patients and nurses will only get worse.
What I read here instead is that the American people is fine with deteriorating healthcare, and will not regulate the industry, nor burst into a walkout of their own.
I find it cheaper to fly back to Europe and pay out of pocket (uninsured) for anything non-trivial along with my flight ticket than pay for California services. Only two things I miss: a) nicely decorated clinics and nurses taking my vitals and information instead of the doctor b) heart attack or stroke chance while reading the bill.
(Of course, I have the advantage of having people to stay with. Perhaps, Airbnb will start offering health services that way soon.)
/s
Seriously, we need to start looking as health care for its value as health care and not a money grab; we pay enough taxes to have a hospital running without the fear of profitability I believe -- in California at least.
Honestly, unless they're not in the midst of fighting a serious illness, most Americans just want to be sure that they have access to better healthcare than the people below them in the socioeconomic ladder. They're fine with healthcare deteriorating, as long as it deteriorates at least as much for the guy below them.
Now, if a serious illness comes along, some people do wake up and realize it's not a f*cking game. But certainly not all.
People here just have inherently less trust in the government providing good services. It has nothing to do with people below them on the socioeconomic ladder. People prefer the devil they know. That’s it.
Well you got my opinion right at least. Distrust in the government is exactly why I have always opposed government administrated Universal Health Care. Deregulation and elimination of most health insurance still looks like the best path, but things are getting bad and at this point I would support anyone willing to try a radical change.
Of course, Medicare already exists. It just only covers the retired and disabled. And while it has its flaws, it at least covers all Americans over age 65. And it's amazing the ferocity with which conservative retirees will defend their government-administered health insurance.
> don't they get more leverage on what QOL and wages they can demand ?
Following up on this apart from my reply above, my observation is instead of raising pay they simply let roles languish. It's bizarre.
But then again it feels like that's what happens when nursing/AP care is treated as a cost center. It seems like they aren't concerned with addressing a market as much as keeping cost/income the same as it has always been.
> It pays far worse than other jobs at the same rate given the effort and stress the job entails.
Depends on location. Most professions I know with that much effort and stress get paid a lot less than $100K, which is the median nurse pay in my area. Amazon pays a lot less.
My point is that you can get a BA and go sit at a decently cushy desk job for 60k-80k/year in many parts of the US. Nursing might pay a bit more but at much greater cost to one's health.
> Amazon pays a lot less.
Yes, I wasn't comparing nursing to jobs with much lower wages.
I was thinking the same as your first point. I'm a career military officer and know a lot of military families[1]. My observation is that the spouses who are doctors and nurses are the only ones who can reliably find middle-class employment. Becoming a nurse is much easier than becoming a doctor, and pays much better than other common things like retail, food service, house cleaning, and photography (probably more of a hobby).
[1] The labor participation and employment rates for military spouses (especially when adjusted for age and education) are so low that they're almost off the charts. The causes are frequent cross-country moves to economically struggling locations, and an extreme need for flexible schedules (e.g. for when service members get deployed and spouses become de facto single parents). Medicine seems to be unique in that it's everywhere, always hiring, and often allows for part-time employment.
Health care is far from a free market for labor, IT, etc. It's one of the most heavily regulated and dysfunctional sectors of our economy. The normal incentives like supply and demand don't work the way they would in other industries.
> Not to be mean, but 'leave nursing' and then what ? Nursing is a well paying middle-class job without a lot of transferable skills to other professions.
Whelp, that the whole point. When you have a good paying job and people are leaving in droves for ??? anything else, maybe even teaching or staying home. That's a bad sign.
To the surprise of absolutely no one who understands healthcare.
I have many friends and relatives that are nurses, MDs, and therapists.
Compensation is about as backwards as you can get. Seniority has no impact on your pay. Once you hit the ceiling you’ll never make more money. This is especially true for Nurses and therapists. Even if you switch jobs. The market rate is what you’re going to get paid (within 10%).
My wife is a PT and made 3x more traveling as a contract therapist than she did as a full time employee. Three times. That’s absolutely absurd.
Benefits are also beyond comical. Healthcare insurance costs for healthcare workers are higher and the benefits are worse than if you just bought Obamacare directly.
Beyond horrible pay with no upward mobility, you’ll also have to deal with completely disconnected management that has never done any clinical work in their lives. They’ll bitch and moan about saving money, and often enforce policies that put clinicians at risk of malpractice. All to save money.
So yeah. If I were to give any young people advice, it would be to stay as far away from healthcare as you can.
Self-insurance seems pretty common anymore. Which amounts to - you can receive treatment in the hospital you work in. You'd at least think it would at least be free, but nope.
I work in tech with no college degree and about 9 years of programming experience. I make mid 100,000's per year. My S/O has 6 years of Emergency Department experience and a bachelors degree and she made about 65k at our local hospital. I think pay is an enormous factor in this. Her local hospital has nurses with less than 1 year of experience being preceptors to new grads.
She should apply for tele medicine. I knew a few nurses that took this on during the pandemic and were making about $50-60/hr from home. I suspect there are fewer opportunities like this now, but it's worth a shot.
How long did it take you to break 100k? Be sure to include those pre-employed years when you didn't even know what 'if' statement meant. A nurse can hit that in 6 years easy through BSN+NP, and that's starting at literally NOTHING. (Alternatively there's a like path for PAs to practice in a mid-level practitioner role that is comparable to NP in those same 6 years)
> A nurse can hit that in 6 years easy through BSN+NP, and that's starting at literally NOTHING.
That NP is the key. Just a BSN will earn you under six figures in most of the USA. We get job mailers because my partner is licensed but non-practicing. And these are advertising nursing positions for $35-40/hr.
According to the BLS, an RN earns an median of $78k a year. $100k/yr is the top 15%.
I spent a bit of time making basic webpages throughout middle/high school using front page. I didn't start taking programming seriously until about early 2013. It took me until about 2019 to hit 100k salary. My girlfriend has 4 years of schooling and 6 years of experience as a nurse. So i guess she has even more total experience than I do.
Anyone can become a nurse. It doesint take exceptional talent or brains. Programming does though. A nurse can't beat a programmer for salary, they're in different leagues
I couldn't become a nurse. It requires hard word, dedication, and focus. I can pull off being a programmer because it provides flexibility.
Saying someone's profession doesn't require "talent or brains" is just insulting. Saying something is "unskilled labor" is one thing, but if you're having a heart attack in a hospital bed, you're going to be lucky there's a person there with some talent at dealing with that (i.e. a nurse).
I never said it doesint require hard work, dedication and focus. If what I did say was insulting they need to get over themselves and their egos are out of touch with reality and thats why it hurts them to read what I said.
It is probably meaningful if comparing to past years.
A lot of people did leave NYC, and probably NYS. So if a much larger number than usual are considering leaving <fill-in-the-blank>, chances are that a larger number than usual will leave <fill-in-the-blank>.
I don't mean to by cynical, but this is kind of my feeling. Throughout the pandemic I saw story and story about nurses getting overworked and being underappreciated. There was lots of talk of a nurse exodus.. and yet it's never happened. Even now it's just talk of a possible exodus. Maybe there are just no similar fields to switch into with comparable pay, but it seems as though nurses are sticking it out in the grand scheme. Are plenty of older nurses retiring? Yes. Are some younger nurses also leaving the field after being burned? Yep. But for the majority of nurses, the pay is still worth all the difficulty they see. Hearing about a co-worker getting attacked by an anti-vax patient is alarming, but until it happens to you you're not gonna make any major life changes to avoid that
About 7 years ago I switched to nursing from nearly 35 years as a software engineer. Each 13-hour shift my 6 or 7 patients, if there was a moment to talk, would ask why I did so. I'd make pretty much the same joke every time: "I was looking a job that was much much harder and paid much much less, so I landed on nursing. Unlike in a hospital, when I was in software and there was a crisis, we'd schedule a meeting and order burritos." The jokes stopped being funny, so three weeks ago I quit my last hospital nursing job.
I did IT support in a hospital for a year. Nurses do everything. Their job is both hard and thankless. I do not doubt satisfaction is low.
But this sounds like the employee satisfaction corollary to Sturgeon’s Law [1].
“90% of employed people are considering leaving their profession in the next year.”
This survey would be more compelling if it compared nurses responses with the general employed population over time. I only skimmed so maybe it does and I missed it.
Thank you for this, the article's conclusion felt very generic, especially after reading the sample group was 200 nurses. Not that Sturgeon's Law is scientific fact or anything, but the observation on it's face rings true. Asking the question alone influences the answer, just like Sturgeon's Law requires an "expert".
While it's anecdote, every single peer in bedside medical care I know without exception has either left the field, or has immediate plans to as soon as student loan debt is repaid. The few older medical professionals in my family are simply sticking out the last few years until they can retire early.
This was generally the case prior to pandemic due to how poor the work environment has become, but the pandemic seems to have broken the few remaining folks who still had hopes and dreams.
How doctors of all professions lost their professional agency to do-nothing administrators within a generation is quite puzzling and a bit terrifying to me.
Having worked in Tech for many years at corporations large and small, I have seen companies run by Founders, by Sales, by Marketing, by Finance, by Engineering, and by Legal. Each had their plusses an minuses.
Until I saw hospital nursing, I had never seen a company run by HR.
Every decision starts and ends with HR. From hiring, to wages, to discipline and promotion, to IT and pay-roll, to reorganization and spending priorities, there is a rule for that. Maybe that rule originally came from the CEO or the CNO, but they say things like "may" and get interpreted as "shall" (or the manager faces a bad review and/or termination) or they are interpreted beyond any rational meaning. My best explanation is that it comes from a fear of litigation and a lack of leadership at the top. The final hilarious story is the CEO negotiating a big deal with lawyers and VPs shaking hands... and then saying without joking, "but I'll have to get HR's approval". The meeting wasn't important enough for HR to show up, but they had the last say.
If you follow the history of HR departments in a lot of modern corporations you often see them operating as private in-house legal firms, and aggressively expanding their purview to include even actions at the executive level. The only thing most HR departments look out for is HR. Everything they do resolves around continuing or expanding the power of the HR department.
Your comment on lack of leadership is spot on. No one wants to be accountable. Instead HR departments put in place bureaucracy that works to deny individual fallibility in the name of a "system of human resource management". They want to treat people like a cog in a machine instead of as people.
That is American corporations in a nutshell. Outsource everything, put layers upon layers, and insulate yourself. Then when fecal matter hits the rotary you can put the blame on others and, at worst, you get fired and there's little to no worry about any sort of legal reprecussion because... well you weren't accountable for the problems in the first place!
It's a massive problem created from little cuts here and there with a few big lawsuits mixed in.
Agree with you, but people on HN and other places tend to flame/heckle companies that don't do this too, aka Elon Musk. Love him or hate him he does things 'his' way without all the seemingly built-in middle layers. I like it as opposed to the HR led office space cosplay, but people seem to want their cake and eat it too.
> How doctors of all professions lost their professional agency to do-nothing administrators within a generation is quite puzzling and a bit terrifying to me.
I have a lot of friends at various levels of healthcare, from nursing up through low and mid-level administrative positions.
The one thing they all seem to agree on is that patient satisfaction surveys have been terrible for healthcare.
Once the emphasis shifted to patient satisfaction, everything became more of a game of catering to what the patient thinks they want. With the spread of rampant medical misinformation on the internet and the rise of alternative-medicine podcasts/blogs/influencers masquerading as informed medical professionals they have a constant influx of patients who show up believing they have a certain condition or need a certain medication. If you disagree too much or refuse to give them the medication they want, you risk a negative review. Too many negative reviews could negatively impact your compensation or even cost you your job.
Even at offices that don't perform patient satisfaction surveys, providers are at the mercy of negative online reviews. Again, if you don't do exactly what the patient thinks they want, you risk scathing online reviews.
This is terrifyingly problematic given the trend of people to self-diagnose with anxiety or infections who show up demanding Xanax or antibiotics. Puts doctors in a situation where they don't really think prescribing those medications is a good idea, but they also feel like they can't deny too many patients or they risk their reputation/bonus/reviews.
It's also a huge problem with conditions like obesity or alcoholism or smoking, where the doctors can see obvious patient-induced health issues but the patient really doesn't want to hear the truth from their doctor.
"The one thing they all seem to agree on is that patient satisfaction surveys have been terrible for healthcare."
My Wife is an ER nurse manager and while you have many self entitled idiotic patients that think they are staying in a resort versus visiting an ER, the patient satisfaction surveys is not very high in regards to the issue and why nurses are leaving.
My wife actually had a person complain that the ER did not have cow bells to call for a nurse (She claimed to be a retired nurse and they always had that for back up, lol) and they constantly complain how come they came in first for a stubbed toe, but another patient with a gunshot wound or heart attack is being seen first.
The bigger issue as why nurses are leaving the field from what she has seen and experienced is:
1. wages: The wages are beyond inadequate in certain nursing specialties and many have left to become traveling nurses or contracted nurses that get paid double the standard nurse pay.
2. Burn out: Besides covid, Hospitals Patient to nurse ratio is often exceeded and no accountability for the hospital to break those ratios. Nor any consideration for a high demand patient versus a low demand patient. Then when something goes wrong the hospital looks to pin it on the nurses. This was an issue before covid . but covid just added fuel to the fire.
3. BS. nurses get bs from ALL sides. They get bs from the patients and even more bs from upper management who set unrealistic process in place that is more concerned by hiding accountability and making things look good on paper than actual patient care. Then you had that whole BS covid movement crap calling nurses hero but besides lip service they did absolutely nothing for them. In fact they did the opposite. I know my wife had to fight the executives because they wanted to make nurses use their vacation time for sick time if they got covid. Their explanation for this that if the nurses got covid it was not likely from the hospital as the hospital takes extreme precautions to prevent it. The funny thing was that the same hospital spewing that BS also wanted nurses to not wear mask due to possible shortages at the beginning of covid. Insert the BS is to DAMN High meme here.
4. RaDonda Vaught's conviction. This is certainly not helping the case to get more nurses.
> My Wife is an ER nurse manager and while you have many self entitled idiotic patients that think they are staying in a resort versus visiting an ER, the patient satisfaction surveys is not very high in regards to the issue and why nurses are leaving.
ER is definitely a different ballgame. Thanks for the additional perspective.
The patient satisfaction surveys apply more to domains where repeat visits are the norm: Family doctor, nurse practitioners, and so on. (Ideally, none of us becomes a frequent customer of the ER nurses!)
Patient satisfaction surveys are the legible feedback mechanism showing that something is deeply broken, but not the source of the problem itself.
It's clear from your comment that the source of the problem is the increasingly sharp divide between what the credentialed medical professionals believe and what lay people believe. The satisfaction survey is simply uncovering that fact.
It would be vastly worse if patients were being treated and had no recourse when they felt their health was mismanaged. It may well be the case that the patients are wrong, but it is extremely dystopian to imagine a world where individuals are not empowered to make decisions about their own bodies.
Patients have always been entitled to make decisions about their bodies. You can decline procedures, and treatment, and you can get second, third, fourth, fifth opinions. Satisfaction surveys do nothing to increase that autonomy. The dystopian world you speak of is a straw man.
The problems stems from people believing they are consumers of healthcare, on equal footing with the practitioner they are seeing. They're not, objectively. A 45 minute Google search doesn't equal 4 years of college (usually in something like biochem but not always), 4 years of medical school, 3-7 years of residency training and potentially another 1-4 years of fellowship training. If you're seeing anyone above a family doctor/PCP, they 100% know more about your condition than you do, whether you've been living with it for a decade or not.
That doesn't mean you don't have autonomy, or that you shouldn't question your doctor's decisions and ask for explanations, but it does mean you should err on the side of thinking the person whose spent at least a decade, but probably closer to two, educating themselves to get where they are probably knows what they're talking about.
> they 100% know more about your condition than you do, whether you've been living with it for a decade or not.
I was with you up until this point. Part of the problem is that this cannot be true in all cases, unless either (a) your condition is commonplace (b) the doctor specializes in your condition.
Yes, doctors know more than you in almost every way about bodies about medicine, about drugs. However, people with relatively uncommon conditions have been enabled (largely by the internet) to create communities of fellow condition-sufferers, and the collections of anecdata that result represent a resource that generalist doctors do not have access to. The good specialists, in some cases, will take occasional dips in to augment their own knowledge and expertise.
Case in point: my daughter has had two major hip surgeries. While there is no way anyone in their right minds would have chosen someone who had not performed these surgeries previously (preferably, many times), and while it was completely clear that the surgeons really really really knew what they were doing, it was also the case that various online communities made up of people who have been through this procedure were able to provide lots of information that the surgeons could/would not. This was particularly true of the recovery process, where there were a number of common oddities that most people who have the procedure experience, and they're really not a problem. They are scary however, and the actual medical professionals really had nothing useful to say about them.
There's another issue with the blanket "doc knows best" rule. If you've had a GP for many years, or a specialist helping you with a condition for many years, then it's probably a great rule of thumb. On the other hand, if you've moved, or for any other reason switched doctors, and you're the kind of person who does pay attention to their body, there's a reasonable chance that you're going to know things about yourself/your body that the new doc(s) will likely not be aware of. They can (and will) learn, of course, and there's no reason to be aggressive or patronizing about it. But for example, you may understand the way you typically recover from antibiotic treatments, or the consequences of lack of sleep, or your tendency to always pull a lower back muscle given certain movements, etc. etc. in ways that your (newish) doctor may not yet be wise to.
> The problems stems from people believing they are consumers of healthcare, on equal footing with the practitioner they are seeing. They're not, objectively.
Objectively, the patient is the only one who has 500,000 hours of experience with the unique and very complicated system we call a body, and is objectively the only one who comprehends what they're feeling. They're also the one who experiences the consequences, they're the only ones with literal skin in the game. How much is all of this worth?
It's a difficult thing. The answer is some mix of giving the doctor and patient power.
The patient already has absolute power. They don't have to accept any treatment they don't want to.
The patient may be comprehending how they feel but that absolutely doesn't mean that they understand the complex interactions within their body, which the physician does know.
That's the theory - That patient satisfaction surveys will uncover the bad providers.
But in the real world, if someone is receiving bad care they don't continue making followup appointments with that doctor. Nobody continues going back to the same bad doctor over and over again and writing negative reviews. It's really easy to calculate churn rate for individual providers.
The hot topic now is tracking outcomes: The idea is that with enough data collection and crunching, we can eventually start tracking which providers have better outcomes among their patients. This is one of those things that sounds great on paper but has a lot of challenges in the real world. It's also prone to gaming, as we've seen from surgeons who have learned to avoid difficult cases so they can avoid the risk of another patient death statistic.
This is spot on. It's not the metric itself which is the problem, but how the metric is interpreted and formed into action. We can all understand the ramifications if we rated parents on "child satisfaction". Lots of kids would be having candy for dinner. The real metric we probably want is improved patient outcome, which may not be synonymous with patient satisfaction.
I don't think that's necessarily incongruent with the OPs point. If the metrics are being gamed or the metrics are being used to inaccurately gauge provider care, those are systemic issues. Or it could be the case of well-intentioned, but poorly chosen metrics.
I get what you're saying, but the promise of the medical system and the implementation of the medical system aren't really aligned. Sure 50% of problems are naive patients, but the other 50% are doctors or a system that doesn't know how to talk to you or treat you, or there's just an ocean of uncertainty in how to operate. You show the negative side from the doctor perspective, but on the other hand. Doctor's aren't really trained in 'health' they're trained in pathology. If you're really sick they can provide help, but if you want to optimize or you're kind of sick, or your numbers are borderline. Medicine is just sort of not a hard science, there's way too much uncertainty. You mention people demanding antibiotics, but the doctor's are just as bad -- last time I tried to have a nuanced discussion about it with a practitioner, the answer was a simple "x days is the standard of care". Not to mention that the doctors would have to be up to date on the latest versions of research in a ton of different areas to have some of those answers anyway. I'm not going to leave terrible reviews about it, but I rarely leave a medical office feeling satisfied that there are firm answers on anything.
I'm friends with quite a few nurses, primarily travel nurses, and not a single one is considering a change in career that I am aware of. Simply an anecdotal counterpoint and nothing more.
They're paid a shit ton more. And because of that, more nurses are quitting to do the travel thing, which worsens the shortage and increases demand for travel nurses ;-) never seen an industry fuck itself over so bad. That's really the issue - healthcare has become an industry, not a profession.
It's really amazing to see travel nurses come back to work at a place they just left. They are now doing the same job as before, are getting paid almost twice as much with better schedules and are working next to people that they know and are friends with.
It's honestly surprising that more haven't taken the jump and is really shocking that hospitals aren't doing more to retain critical staff.
Its hilarious that nursing shares this problem with the tech industry and probably with most other industries. Every company is extremely allergic to giving raises and is happy to let their workforce churn constantly. You would think they believe that experience has no value.
But on the hiring side, experience is one of the most widely accepted signals of value.
1. Hospitals pay their nurses $X, which is way too low
2. Nurses quit because they're underpaid and overworked
3. Hospitals have a nurse staffing crisis and so pay travel nurses 2 * $X (or more!)
4. Hospitals are in a panic over the cost of travel nurses, yet instead of paying their nurses more to keep them around and eliminate the need for travel nurses, they ask the government to cap the cost of travel nurses
My mind is exploding over the ridiculousness of it.
Then increase the pay even more or increase the quality of life at work.
Instead of $250k, halve the work load somehow and make it two $125k.
If there is no number, then society cannot afford it.
But this is nursing, not trying to find ways around the 2nd law of thermodynamics. If nurses received $300k/year income, then there probably would not be a shortage since the barrier to entry is not that high.
If we really want to get down to the nitty gritty of it, most people cannot afford quality nurse care (or doctors or hospitals). So the question really comes down to how much wealth is society willing to redistribute to those who need it in the form of healthcare?
The point is that I know nurses that make 200k a year and still complain about the workload. More nurses and better hours is the solution. Meanwhile the trend is to make it more and more difficult to become a nurse and higher and higher for hospitals to have nurses
Not even close if you are talking about the USA (and actual nurses, not CNA's or MAs) - starting pay for 2 year RN degrees near me are about 55-65K, and you easily go over 100K in a few years.
While technically true, what we're trying to avoid is forcing the market to find a way that may include an interim period of extremely bad outcomes before correcting itself
A travel nurse means you just have to work across town you dont have to travel out of state, out of country, or to middle of nowhere. And these people are bringing in 5k a week currently. None of them are leaving.
Funny you should mention that… reading all of this, I was thinking of a podcast interview with a nurse who was retiring from hospital work. His primary reason for leaving was being tired of fighting with hospital ownership and administration, and was planning on switching to travel nursing which appears to be more of a "gig" space.
He did consider that a career change, I think in the same sort of way that a computer programmer like (presumably) most of us would consider quitting Google to work on an indie app or videogame development would be a career change.
The larger point is, medical professionals are bailing from the hospital system, which looks pretty busted.
I can add another data point. One of my mother's friends works as a travel nurse. I don't envy her lifestyle, but she seems to find that the compensation makes it worth her time.
The other responder said the same thing, but to add, a traveling nurse I’m friends with , in Texas, gets paid 5k a week if he chooses to work and chooses where he wants to work. So again, this is like making a judgment about software development working conditions by using people rest and vesting at FAANG as an example.
The travel nurse market is growing due to supply and demand problems.
The demand for nurses is increasing as people are leaving and there are more from the boomer generation hitting an age where they need more care.
The supply has stayed the same. Schools local to me have not increased output for various reasons (lack of instructors, lack of space in local hospitals where nurses train, etc). The supply is too low.
So, we have a supply and demand problem. Travel nurses get paid a lot more because of this.
The solution is to produce more nurses. Something few are talking about.
One of the local schools, to me, turned away half of applicants because the program isn't increasing capacity.
No, the solution is to pay nurses better. There are already tons of high quality nurses who don’t want to do it anymore because of poor pay in the face of demanding hospitals and patients.
Poor pay? Judging by the nurses I have talked too in big proper hospitals stress and scheduling are their main concerns, not pay.
Obviously higher pay would increase their abuse tolerance, but I think it is only part of the problem and a short term solution since no amount of pay will offset stress problems.
County level nurses seem to have much better work conditions than hospital nurses.
But, before COVID there was already a supply problem. The supply problem has been slowly getting worse for years and then COVID accelerated it. If every nurse came back to working as a nurse who wanted to work there would still be a supply problem.
Supply has not been growing to meet the demand growth for years.
I suppose you could just pay people more money to make it worth it but the long hours take a toll in other ways as well and contribute to burnout no matter how much you get paid.
> lost their professional agency to do-nothing administrators
You just summarized the decline of Western civilization in one phrase.
This has happened almost everywhere and efforts to push back have proven extremely difficult. I personally place a lot of the blame on the educational system for overproducing administrative skill sets and underproducing practical skill sets. There is some role for those things of course but we have far too many people for the administrative roles we really need and far too few for many other professions. This combined with the tendency of people to recruit people like themselves has oversaturated the market with administrators looking for reasons to exist.
The rot is to the point that we have the spectacle of Elon Musk looking like superman. Why does he look like superman? Because he actually does things instead of having meetings to discuss the meeting schedule. He's just a reasonably competent engineer and business founder with huge resources who... does things... and this makes him look superhuman by comparison to the hordes of administrators that only discuss doing things and commission studies about hypothetically doing things.
Pretty much. Unfortunately, we've also created a massive underclass in the West who have effectively no applicable skills. They can neither administrate, or do things, and so they are effectively dead weight on society. Ironically, considering that administrators are driving us over the cliff, the underclass is less problematic than the administrators. At some point we'll hit a critical mass and there will be so few people left that know how to do things that we literally will be unable to maintain the basic infrastructure of civilization. The cracks are already starting to show.
The sad thing is that this is so very obvious, and yet such an intractable problem to solve. The entrenched systems at every level of society will fight you at every turn when you try to improve things.
See also: California’s plan to eliminate algebra 2 and calculus from the highschool curriculum. It is being spearheaded by someone without a math degree, in the name of improving marketability of the kids for data science positions, or something.
See also (2): Monty Python’s bicycle repairman sketch.
> in the name of improving marketability of the kids for data science positions, or something.
They have been very clear and upfront about the goal. They want to "solve" racial discrepancies in graduation rates so they've taken the classes often failed and are removing them.
For a while now it feels like the left and the right are attempting to one-down each other on how stupid they can get. That proposal seems like an example of the left trying to out-stupid Trump and the alt-right. Don't worry I'm sure the right is working on things even dumber than this, and then those will have to be topped, and so on. In 2024 we will have Dr. Oz and Marjorie Taylor Greene running against Oprah Winfrey and Kamala Harris.
I'm not sure how this downward spiral ties into the administrative position over saturation problem, but I have the intuition that it does somehow. Maybe what we have are a whole ton of people who don't really know how to do things who vote. Voting is ultimately a hiring decision, so what we get is a voting process that hires a whole bunch of either administrators who themselves don't know how to do things or crackpots because people without practical knowledge can't spot a crackpot.
> Burnham’s claim was that capitalism was dead, but that it was being replaced not by socialism, but a new economic system he called “managerialism”; rule by managers.
That is an interesting observation. I wonder how much of the advent of "talking over doing" is related to the development of mass/social media.
Influence can propagate so easily through mass media, meaning that it is now possible to generate enough business interest just through "hyping" (it's difficult to achieve this when messages have limited reach) --- combined with the fact that it is often cheaper and less risky to "talk" than to actually "do", we end up with a culture where hyping is preferred whenever possible.
It's not about Western civilisation, it's about economic neoliberalism, replacing every existing metric with a single one: shareholders' profits. Those do-nothing administrators _do_ have a marketable skill: they make money for the company. Or at least appear to, according to (obviously flawed) criteria that are being used to evaluate ones' work.
> How doctors of all professions lost their professional agency to do-nothing administrators within a generation is quite puzzling and a bit terrifying to me.
I would bet it's caused by:
- stifling bureaucracy
- hostile legal climate
- massive start up costs
The only winning move is not to play. Let the system fall apart and join on the later upswing. The unfortunate part is all the needless suffering people will endure during this process.
Both my mother and sister were nurses and disenchanted with the profession (in Switzerland) long before the pandemic hit, as the hospitals got completely mba'd during their careers.
Whereas in the past they could actually take time interacting with patients, now everything needs to be Lean and it's just about shoveling people through the system with minimum resources while extracting ever more money. I don't see how this can end well.
My mother switched to an administrative role internally, 10 years before she got retired and my sister went from nurse to anesthetist and now in the progress of moving to IT as a domain expert for medical software so she can work from home.
> How doctors of all professions lost their professional agency to do-nothing administrators within a generation is quite puzzling and a bit terrifying to me
This should terrify everyone. Large segments of our society are failing us despite being stuffed to the gills with administrative staff that don't contribute much to productivity but rob professions of their independence. We're managing ourselves to death.
Yes. The system is gross. When my dad suffered from a stroke (pre-COVID), the level of neglect and poor care he received was startling. He died before he should have after making substantial recovery due to the side-effects of being in a hospital.
My mom was a long-retired medical director of a hospital and even she was shocked at poor quality of care, compassion and competence. Even in the ER of a recognized trauma center, things were pretty meh. Some specialist floors and ICU were good, but when an infection caused by poor hospital hygiene struck, he was relegated to the “medical” floor, where he was not fed, medicated, turned or treated with respect. Ultimately we maintained a 24x7 staffing of family volunteers for over 6 weeks.
Many of the staff frankly sucked. But it was easy to see why - the staffing levels were so poor pre-COVID, that any RN risks license every day by virtue of being there. The smart ones GTFO. You can’t care for 15 patients.
I frequently say that administrators have killed both the education (esp. tertiary) and medical fields in the US.
I’m pretty sure both of these will implode under the bureaucratic weight at some point — the financial and social costs of the excessive administrators is not justified by their (often minimal or negative) value added.
Yes, it's like someone held up a mirror when you look at what has happened in Higher Ed when the professors stopped running things, and Health Care when doctors stopped running things. Costs skyrocketed, outcomes stagnated or declined, satisfaction plummeted.
My frame of reference on this topic is that my family is mainly medical doctors and I started and run a yc backed Series A stage startup.
In my experience, the administrators are often doctors at hospitals and people all the way to the top have to have strong medical backgrounds. That's not to say there aren't do-nothing administrators, but those do-nothing administrators are often doctors. They tend to adhere to the way things are and always were as an orthodoxy, like 1st year residency is the worst and at these points quality of life improve, but it's almost like a fraternity hazing justifying the insane hours, complete loss of work life balance just because this is how it is. Candidly, there does seem to be a guilty pleasure there.
There is little to no real discussion on how to improve not only the work conditions but also the user experience of medical care. In my view, it starts at the top; organizationally, they are lacking an entire skillset to make any improvements what-so-ever.
Everything is controlled by insurance companies. You can’t do anything unless it’s exactly how insurance wants and only for what insurance will pay.
It limits everything, including how every profession can be compensated simply because you can’t easily hire somebody for more than what insurance will pay for their services. You can, but the funds have to come from somewhere.
Insurance is the only industry where they agree to pay for something (in this case, "medical care"), but then after service has been rendered can decide to pay less, or not pay at all, or stop paying that provider altogether, etc. This combined with hospitals being run by non-physicians*, and people thinking being able to Google and read WebMD qualifies them to argue with their doctor about treatment plans**, healthcare in the US is going to absolute shit***.
* I strongly believe that only physicians should be running hospitals. Certainly not administrators whose only education is an MHA and only experience is working for for-profit health companies. Medical decisions need to be made outside of cost considerations. The only factors should be medical science, quality of life, and patient wishes (in that order).
** In stark contrast to asking questions and trying to understand. But I have family members who are the "look everything up and then try to tell my doctor how they're going to treat me" ilk and it's crazy.
*** I don't think the above points are unique to US healthcare other than cost considerations, but that's all I have experience with.*
As a quick counter-point to *, there is another sub-problem with healthcare/doctors in the US, where often patients with chronic illnesses or not-easily-testable conditions have to fight hard for doctors to take them seriously. The why of this varies a lot from what I've seen, but includes:
- an attitude of "most patients are just trying to wring medications out of you"
- an ego-hit of "if I didn't make the diagnosis, I don't want to help" (this applies to both patients coming in with a suspicion of what they have, or getting a diagnosis from another doctor)
- burn-out/overworking, where doctors have a hard time managing all the different cases coming at them without dropping the ball here and there
It's not a simple, single-cause problem at all, but just want to provide an alternative point of view about patients who look things up or come in asking about a specific condition or diagnosis.
When I got my ADHD diagnosis after a quarter-century, I went in specifically asking about ADHD because I had seen some flags that made me think I might have ADHD. Contrast that with the people doctors screen out who are trying to get a stimulant prescription despite not needing it, and you have a situation where it's hard for doctors to tell who does or doesn't need meds, and where patients with actual conditions have to fight hard for those to be diagnosed.
Even in cases like POTS, which has no medication involved in treatment, just lifestyle changes, and yet people close to me who have POTS all had an uphill battle getting it recognized by anyone, especially doctors who could diagnose (disclaimer: sample size = 3).
> When I got my ADHD diagnosis after a quarter-century, I went in specifically asking about ADHD because I had seen some flags that made me think I might have ADHD. Contrast that with the people doctors screen out who are trying to get a stimulant prescription despite not needing it, and you have a situation where it's hard for doctors to tell who does or doesn't need meds, and where patients with actual conditions have to fight hard for those to be diagnosed.
I told my doctor I had already been diagnosed with ADHD because I had a strong suspicion I had it and wanted to see for myself if the medication helped (it helped massively). I think medicine should be accessible for patients who need it but I don't know how to avoid large amounts of patients then taking medications for the wrong thing, which would probably happen if it was a free-for-all. It kinda comes down to the question of having the personal freedom to hurt yourself doing something stupid, which is a balance (a little of that freedom is good, too much probably bad). All-in-all I lean toward the current system of using on experts to make the final decision. Still, I would be really pissed if a doctor prevented me from getting stimulants for something I believe I need, so I am not 100% satisfied with the current system either.
Another wrinkle to the problem with that gatekeeping structure is that it is so prone to bias against women and people of color, who are much more likely to be undiagnosed and ignored or dismissed.
> a 2000 study[0] published in The New England Journal of Medicine found that women are seven times more likely than men to be misdiagnosed and discharged in the middle of having a heart attack.
> women with chronic pain conditions are more likely to be wrongly diagnosed with mental health conditions than men and prescribed psychotropic drugs, as doctors dismiss their symptoms as hysterics [1].
> racial bias in pain perception is associated with racial bias in pain treatment recommendations... Black Americans are systematically undertreated for pain relative to white Americans.
(To contextualize the votes: I think you were getting down voted for assuming that sexual and racial bias don’t exist. You assumed the statement mentioning that such biases existed was inaccurate and wanted explanation as to how. However, per my other comment, the biases exist and contribute to significant negative health outcomes for the disadvantaged groups.)
I view drug enforcement policy meant to prevent individuals from making decisions for themselves as always doing more harm than good. The place for regulation in this space is controlling what claims profit-motivated entities can make about drugs, enforcing quality and safety standards in manufacturing, and honestly tying the hands of insurance companies as much as possible, if not just gutting them altogether
Yeah, I've witnessed this first hand with my spouse. She's been told she just needs to exercise more (she was a professional dancer when it hit her), that it's all in her head (actual psychiatrist said otherwise), that it will resolve in 6-18 months (it didn't), etc., etc. It's pretty appalling.
Thanks for mentioning POTS, btw. Despite how many people have it, it's still fairly poorly known about even within the medical community.
I'm more and more convinced that POTS/EDS/MCAS aren't rare diseases, they're just criminally under-diagnosed because they tend to affect women. FWIW, POTS is much more manageable with medication (e.g. Midodrine and Florinef).
> criminally under-diagnosed because they tend to effect women
I just can't understand this argument. Women already live 5 years longer than men on average. You mean to tell me if the system didn't discriminate so strongly against their best interest they'd live even longer than men?
Responding to both you and the comment above/below you:
Women have a hard time getting symptoms, esp around pain, taken seriously. Oftentimes these symptoms are downplayed or ignored, regardless of the sex/gender of the medical professional.
nurses are 91% female and doctors are about 37% female - are they also 'criminally under-diagnosing'? Seems there are quite a few more women in healthcare than men these days.
The counterpoint to your last thing is that there are also many ailments that we literally just do not have enough info about yet to have proper treatments. And if we are studying such things many doctors are not going to always be up on the latest research for that specific condition.
I have found it helpful to approach it in more of a teamwork-like mentality. Don't just read WebMD and try to diagnose yourself - journal your symptoms, observe the trends, record data. If it seems like it points to a specific condition hop on Google Scholar and look for some legitimate new research the average doctor may not have heard about. Print that out and then when you go in show them and ask questions without attempting to specifically diagnose yourself.
You could be totally wrong but with some background info your doctor is much more likely to accurately diagnose and take you seriously.
> people thinking being able to Google and read WebMD qualifies them to argue with their doctor about treatment plans
In my experience, I have had:
1. Doctors that know nothing about a really basic ailment and not have any meaningful guidance or treatment to suggest
2. Doctors that Google something literally in front of me, things that I have already Googled myself, and draw the wrong conclusion because they're looking at results at a glance - when I had searched myself earlier and dug deeper though, it was clear to me the result he was looking at was just plain wrong
3. Doctors that provide very little to no guidance about a wide selection of medications available to treat a problem, leaving me to essentially guess which option of a dozen or more I should go with
4. Doctors that force me to advocate for myself and my condition before they agree to help treat it - so much so that I had to visit 4 different doctors to find one that would, wasting nearly a thousand dollars of office visits with nothing to show for it.
It's no wonder people do their own research and dare to advocate for themselves. Most doctors are fucking worthless.
I felt the same way until I started being more active in choosing quality doctors. Doctors are no different than any other profession - there are the ones at the bottom of their league that are just going through the motions and there are the superstars working for some of the best institutions in the world. The key I have found is to specifically look for doctors that are either actively involved in academic research pertaining to your ailment or are working at quality institutions that are engaging in research that is at least tangentially related to your issue.
Keep in mind they also have to do a stupid amount of paperwork these days for every patient and the place they work for may be overscheduling the crap out of them - generally (unfortunately) I always consider my first appointment to be sort of a wash due to this and assume I am not going to really get anywhere until the second time I see them.
I cannot agree enough. I think anyone who has dealt with a puzzling condition quickly learns how limited the "expertise" of these supposed authorities is. Sure, insurance companies are terrible, but so are most doctors. Great, quit, you probably sucked anyway.
It also probably doesn't help that doctors are jacks-of-all-trades medically - there are simply too much complexity to thoroughly understand the nuances of every obscure condition and interaction.
However, I think acknowledging when one doesn't know something is a skill many could benefit from improving...
just adding a case when a doctor prescribed double the quantity for an infant. i spotted it right away, he panicked, asked to have the prescription back and promptly destroyed it.
> * In stark contrast to asking questions and trying to understand. But I have family members who are the "look everything up and then try to tell my doctor how they're going to treat me" ilk and it's crazy.
I still think it’s better than the other extreme of just showing up and trusting the professionals. That should work in theory, but my experience for myself and those around me is it’s incredibly ineffective. If what you’re dealing with requires the least bit of thought, odds are you’re getting brushed off to the extent you allow.
The real model of US healthcare is essentially apprentice/master, with the patient as apprentice. Apprentice does a lot of the work, not all, some needs to be approved by the master and the apprentice better know how to learn from the master, when to push back, and how to make it seem like it was their idea all along. You can imagine how this falls apart for mental health.
I also think the complete implosion of family medicine has made this worse. In the past, you would keep the same family medicine doctor for decades and trust them. They in turn would know what your values and priorities are. Moreover, they would be able to guide you through difficult healthcare decisions that inevitably come up (cancer diagnosis, mental health etc.). We have lost the human connection aspect of medicine and those few physicians that are able to hang on to it are burning out due to the massive amounts of paperwork they need to accomplish. From the hospital perspective, (which many physicians now work for) good paperwork=good patient care. Paperwork is measurable. Relationships (other than in the abstract) are not.
> * I strongly believe that only physicians should be running hospitals. Certainly not administrators whose only education is an MHA and only experience is working for for-profit health companies.
The skills need to run a hospital are quite different than those required to be a doctor. I'm not saying hospitals aren't unique - I believe they are and their adminstration is highly specialized. Doctors should inform the administration at every level but it would be a waste of their training and a bad idea for doctors to run everything.
> Medical decisions need to be made outside of cost considerations. The only factors should be medical science, quality of life, and patient wishes (in that order).
Would you be as quick to say "Doctors should work without pay." ?
Why would not paying doctors be the natural consequence? It’s a fairly significant jump to go from don’t let cost be a primary decision driver to let’s force doctors to work without pay.
Because in reality, there are always tradeoffs and constraints. In the US, a disproportionate amount of healthcare costs come at the very, very end of life.
It's possible to meet the sole criteria of science, quality, and patient wishes with exploding costs. I think the OP's point was that money has to come from somewhere.
"a disproportionate amount of healthcare costs come at the very, very end of life."
One might ask why that is; while some is surely due to natural decline in later years, one could likely also posit that the cost-fears leading up through that period (decades), and the general inability to get people to do preventative care throughout adulthood contribute to that significantly.
It is one consequence of a highly atomized culture. I suspect it happens because individuals are expected to take responsibility for their care (basically, this is the human side of cost-shifting and corporate planning around the care gradient available to someone at a given wealth level).
To someone at the end of their life, money is usually less interesting to them than a few more days of breathing. So the market provides.
The explanation I've heard is that it's rooted in the cultural sanctity of life and how that translates to trying to preserve life at any costs (even when quality of life is no longer present).
To be clear, I'm talking about the absolute twilight of one's life that's reached regardless of levels of preventative care. I think there's potentially an opposite point that could be made: taking care of one's self can prolong this period and make it cost more. Someone who drops dead of a heart attack one afternoon won't have the same end-of-life costs as someone who gradually becomes enfeebled with age.
We’re “fixing” this by flooding the market with less trained nurse practitioners and PE. Doctors are being gobbled up by regional medical cartels and put where they can maximize billing.
>>We’re “fixing” this by flooding the market with less trained nurse practitioners and PE.
In reality though, the overwhelming majority of cases that walk into a doctors office on any given day do not require an actual MD - NP and PA's are more than capable of handling many, many things that a typical patient needs.
Everybody tends to think they need a 'real doctor', they usually don't. Its good they are there when they are really needed, but do you really need an MD to diagnose a sore throat, adjust your BP meds or many other routine things that are people are seen for everyday?
> The skills need to run a hospital are quite different than those required to be a doctor.
And still, in many countries, including highly industrialized ones, hospitals are run by doctors. So either US administrators are making their hospitals run a lot better (which does not seem to be the case), or the core incentives each group optimizes for are different.
It should still be doctors. Just makes administration a career path that a doctor can choose to move into. There would be plenty of takers from the ranks of those burnt out on patient care. They could even find new meaning in being able to help people without going through the bedside wringer. If professional administrators have a place in the system it’s in positions under experienced physicians where they can help with implementation of policy, not shape it.
> The skills need to run a hospital are quite different than those required to be a doctor.
Why do you think law firms and accountancies are partnerships? Because the best proffesional for managing lawyers/accountants/develipers is such a proffeshional with loads of experience. Thats why we have progression, you gain management skill as you bevome more senior but you still know how the industry works and the people you manage
No, you first find people who want to go into management, then you give them management responsibilities without promoting them until they prove they can handle it.
> I strongly believe that only physicians should be running hospitals.
This is how it is for other professional industries. As an attorney, you can lose your license for sharing any profits with someone who isn't a lawyer. I believe states typically require accounting and engineering firms to either be wholly or two-thirds owned by such professionals as well.
Why shouldn‘t money from law be kept in the hands of lawyers? It‘s a grueling education with an even more grueling exam and even now a lot of law graduates can barely afford to keep a roof over their head
Because the profession is meant to serve the public interests and not just be a money grab. According to government data, the median lawyer is in the top 10% of income earners.
Correct. ONet data puts the median lawyer at about $127k. From what I could find, 90th percentile of income is around $126k.
While I know HN is probably SV and software biased, saying "only" $120k comes across as out-of-touch for the way most people live. For comparison, the median SF lawyer makes $191k according to BLS data. I could not quickly find 90 percentile data for the area.
Your average Enterprise CRUD developer in any major city in the US can hit that number within 3-5 years and a job hop. It’s not exclusively a SV thing.
And your number is correct according to Census data.
I agree, but it's still out of touch. (not a knock on you, we are all subjectively influenced by what we come into contact with the most and interpreting it as 'normal'. It's also why something like 90% of people consider themselves middle class.) The fact that you have to narrow it down to software development and major cities should tell you that much. That's also why my original comment included both SV and software as biasing factors.
The average person does not develop software and does not live in a major city. If somebody is making double the median wage and 2.5x the average wage and complaining about keeping a roof over their head, they can probably expect some sideways glances. It's like when people complain about the difficulty of making ends meet once they make their Lexus payment and pay their kids private tuition bill. The subjective struggle may be legitimate but it's still out of touch with the experience of most people.
Many states of laws regulating the "corporate practice of medicine." But it seems like that leads to a hospital just being bunch of loosely held together independent businesses/contractors.
I'm pretty sure no jurisdiction allows lawyers to share their billable hours with their support staff. You have to pay them either hourly or salary, not linked to how many hours you're billing. You can't give them a law firm stock package or say they get a 10% commission on all billed revenue or something. At best, some jurisdictions allow law firms to give an annual bonus if the firm does well.
I feel like the person you are responding to was not meaning software engineering. Electrical engineering, Chemical engineering, Civil engineering, Mechanical engineering, etc are all more likely: especially as what you say about software engineering is definitely well known.
Now, I get we like to refer to ourselves as Software Engineers, but surely you understand he means actual certified engineering firms, not groups of code monkeys, right? Software is virtually never engineering, you'd have to get to a situation like flight control software before you're doing anything legit
If you have never stepped into a domain where you have to formally verify your software, I think you should probably not take too much offense to such a comment. While I admit it may be slightly negatively connoted, I primarily used it to illustrate that the kind of engineering going into making a bridge differs greatly from making your UI widget pixel-perfect or your SQL query from being too polynomial
I believe this is in reference to Professional Engineering firms, which often requires PEs either as owners or in certain roles. As far as I'm aware software engineers are not required to be Professional Engineers in the US for most tasks, nor are SaaS shops required to be licensed as Engineering firms.
NCEES did toy with the idea of a software engineer Professional Engineer license, but it went away due to too little interest. I think it was in part that industry didn't want it because it would give more leverage to SEs. IMO the only way that will become commonplace is if it is forced by regulation.
> insurance is the only industry where they agree to pay for something (in this case, "medical care"), but then after service has been rendered can decide to pay less
That's not always the case. The reason I stopped writing mobile applications long ago was because the mobile carriers were doing exactly this, and not even providing enough paperwork for you to argue with them about it.
People like to lambast the Apple App Store for being greedy, but the fact of the matter is that people netted 3x as much off Apple that they did from the carriers. They are asking too much money now but their rates were absolutely defensible at the time. It's not a coincidence that we had a gold rush that started almost exactly when the App Store became a viable target.
One might ask what would happen if we joined the rest of the 1st World in providing medical care and marginalized private health insurance. Would it be a similar watershed moment?
The "only physicians should run hospitals" doesn't make that much sense to me. Reminds of the technocratic argument you used to see a lot on the internet that instead of politicians we should have scientists and engineers in legislature.
The issue is if you have someone with a scientific background doing politics, what you have at the end is still a politician. Same thing here. An MD doing hospital administration is an administrator.
Which is not to devalue specialist expertise in these roles. I definitely think you want people with these backgrounds in those roles as well. Just not necessarily exclusively. A career administrator has different skills than a physician, you want people with both, and other, roles working to run a hospital.
The real problem as I see it is probably the incentives, constraints, and pressures they work under, or towards. A physician forced to run a for-profit hospital maximizing returns is going to make a lot of the same decisions as someone with a business background in the same situation. The thing is to change the situation, not put different people into that role and expect them to do it dramatically better.
Works pretty well for lawyers. It's not perfect, but lawyers have to adhere to a code of legal ethics, and only lawyers can have equity in law firms. Seems like this model could be transferred directly to the medical industry. It would not solve every problem ever, but it is an interesting thing to look into.
Yeah that sounds fine too if you can do it. Anything that prevents hospitals from being operated by large profit-seeking entities with no other stake in them would probably be a strict improvement over the current system.
I think the practical issue is those fields that have similar restrictions basically predate a major societal shift. We now consider the only valid limits on profit and ambition to be market forces. I'm not sure restricting hospitals in this way is less radical than just nationalizing them, in terms of practical politics.
Anyway, again, sure. I'm not informed enough on this subject to know what model would actually work best. I think the problem is the raw exclusive profit motive rather than who specifically is running them, but there are a lot of ways to eliminate that.
There might be a parallel to a medical group or a professional corporation, but a law firm is a vastly simpler operation than a hospital. Orders of magnitude simpler.
The problem with this is that the MBA programs that churn out hospital administrators tend not to be very good...focus on mergers, cost cutting, not so much on optimizing care. The pendulum has swung too much onto the MBA for MBA's sake hospital administrators and less so on actual medicine.
> A physician forced to run a for-profit hospital maximizing returns is going to make a lot of the same decisions as someone with a business background in the same situation.
Indeed! Whereas a doctor might say yes, give that patient with cancer the treatment they need, the MBA is going to say no, it costs to much, let them die. If the goal is to maximize profit, the MBA is doing a better job. If the goal is to maximize the health of your patients, the doctor is. We must realize that these two goals are fundamentally in conflict with one another.
The question isn't whether a doctor or an MBA should be running a for profit hospital, it's whether we should even have for profit hospitals. If we care about people more than profits, then clearly we should not.
At some point, you have to put a value on a human life.
It sucks and no one likes it, but what is the alternative?
Each human life is worth infinity? So we should bankrupt the entire country, spending 10 trillion dollars on a surgery that has a 1% chance to save a 98 year olds life?
Obviously that is an extreme example.. but the point is sound. We only have so many resources, how do they get divided up? Should be spend millions to give 80 year olds 1 more year of life? Do we value life on the reverse of age, so a baby we value at 10 million dollars, but a 90 year old we value at $20,000? What if that 90 year old is your Grandpa?
> So we should bankrupt the entire country, spending 10 trillion dollars on a surgery that has a 1% chance to save a 98 year olds life?
This is a pretty wild straw man fallacy, but I'd like to give a good faith response nonetheless.
You may not know, but the US spends more per capita on healthcare than any other country in the world, by a longshot. Many other countries provide unimpeded treatment for all of their patients. If a doctor in Japan wants chemo, the patient gets chemo, and treatment starts immediately. So how does it make sense that we spend more on our patients but doctors are still told no, the patient can't have that treatment? It's because a larger share of our biggest-in-the-world healthcare spending goes to for profit companies, like insurance companies, than anywhere in the world.
So when an insurance company says no to a treatment, it's not because we don't collectively spend enough for that treatment, we do! It's just that the insurance company wants that spending for themselves.
Spoiler alert -- the author being interviewed doesn't have a solution, quick, easy or otherwise. But the history is fascinating -- in the end there are a lot fewer villians than you might imagine. A lot of good faith decisions seemingly made in the public interest over the past 150 years have led us into a weird local minimum that seems inescapable. Where we are was not inevitable, and as they say if something is unsustainable it has to end eventually, but before suggesting sweeping solutions I'd recommend hearing a detailed history.
Let's not be obtuse though. The majority of healthcare costs are incurred at end of life. Perhaps insurers and the government should not subsidize any life saving care for those over the average mortality.
I know for example, my grandmother who lived in europe many years ago, had failing kidneys. While today it's likely she could have subsisted for more years on dialysis, perhaps that money didn't need to be spent.
Life is finite, and racking up bills at EOL is a waste. People need to learn how let others die with grace, instead of giving chest compressions to a 85 year old 80lb grandmother.
You didn't address the scenario as presented, or demonstrate how it violated a principle you had described. Instead, you shifted to excoriating the insurers for greed and waste.
Should the insurance company bankrupt itself on the first client? If not, how should they decide how much to spend on each? I should note that non-profit hospitals have similar results as for-profit hospitals (in the USA), so there's little evidence of shareholder greed playing a significant role (though there are many other stakeholders including employees).
We already have decent (not always great but decent enough) government provided healthcare for the elderly through Medicare. So in fact, we've completely avoided your example already and said "yep, all life has value if you're eligible for medicare".
Of course resources are finite, nobody ever argues that they're infinite. But we treat healthcare as if there's a constant scarcity of medicine with how much is charged because there's a constant urge to squeeze even more profits out of patients who probably have only 2 choices- pay for the medicine or die.
The counterpoint is that you have the exact same decisions being made in systems like the UK. People get refused cancer treatment because they were too old and their were younger patients that had a better prognosis. The fact is both types of systems don't have unlimited resources.
Yes, care rationing is a thing. But in the UK care is rationed due to capacity constraints whereas in the US it's rationed in order to make a profit. These are very, very different things. It means that people's welfare, and death, is being traded for profit.
re: "Medical decisions need to be made outside of cost considerations."
In the end, labor hours of professionals are finite. Even if you don't need to pay doctors, you only have so many, they can only work so many hours, you will need to prioritize who to help in what way, which procedures to do. Same with all the other personnel, the consumable stuff, the devices/scanners/equipment, etc. So someone is going to have to prioritize. It can be just "how much quality of life can we save using the resources we have", regardless of the patient's ability to pay/insurance/citizenship, but some prioritization will need to happen. The policy of the death panels can be changed, but their existence is inevitable.
This is why it makes no sense to have doctors and nurses waste time battling insurance companies over treatments, and hospitals over staffing. Their time is indeed too valuable.
This is exactly why we should simply just expand medicare to be an option for everyone. If it's good enough for everyone over 65, it's good enough for everyone under it too. I'm ok with paying a reasonable premium to have access to the largest insurance network in the nation.
Simply? It is not so simple. Medicare reimbursement rates are way below commercial rates and hospitals wouldn't survive just from medicare reimbursement alone.
Let's stop trying to come up with "simple" solutions to the healthcare catastrophe in the US because the reality is more complex.
So raise the reimbursement rates to the point where hospitals can survive, or cut the fat. See? Simple.
Every time someone makes an argument like this, it's always to say that somehow, medical treatment in the USA is special compared to other countries. We couldn't possibly have universal healthcare work here. Please.
Possibly misattributed, but usually given to HL Mencken:
"For every problem, there is a solution that is simple, neat, and wrong."
Don't kid yourself into thinking a complex system that makes up 20% of GDP is going to have a simple solution. Just a couple examples you'd have to contend with:
1) Insurance companies get a say too, according to the Constitution. That means they get to lobby in their own interests. That political problem itself is a boondoggle.
2) The US funds a disproportionate amount of medical R&D. Some of that fat is going to be cut from research. You need to have a plan on how that will effect long term quality of care and innovation.
3) Physician licensures are limited by the AMA. If you expand coverage, you will need to expand supply because any time something becomes "free", people will consume more of it. That's not a necessarily bad thing in healthcare, but needs to be addressed. The AMA also gets to defend their political interests.
There's lots and lots of other issues. I'm not claiming the US healthcare system is great. But pretending it has a simple fix is naïve.
Again, I point to the fact that nearly every other industrialized nation does it better than us, with a fraction of the resources. I find it highly suspect when people say the problem is so complex we can't possibly fix it. Every other major western (and some asian) economy has addressed this. We are not exceptional. We can fix this too.
Yes, but that is, in part, because the US effectively subsidizes other countries medical R&D. Similar when other countries cap their drug costs while the profits are made up within the US. That means we subsidize other countries healthcare costs at the expense of our own. A country-to-country comparison is incomplete without understanding those systemic issues.
It's like when people point out how much the US spends on the military compared to other Western industrialized nations. Part of that discrepancy is due to the fact that the US disproportionately funds organizations like NATO. Other countries reap the benefit without footing the bill. There was a lot of outrage in Europe when the US tried to enforce the NATO GDP spend that other countries already agreed to.
The US can do better, but I would argue we can't unless we fully understand the complexities of the system. That means not getting enamored by the idea that there are simple fixes. The first step IMO is getting the political will to do so (and to understand the tradeoffs within a complex system), because many of the potentially solutions are stymied at Congress.
> Medical decisions need to be made outside of cost considerations.
A common attitude which may cause:
Health care is extremely costly in the United States. Although the rate of growth in spending has attenuated in recent years, per capita spending on health care is estimated to be 50 to 200 percent greater in the United States than in other economically developed countries. Despite leading the world in costs, however, the United States ranks twenty-sixth in the world for life expectancy and ranks poorly on other indicators of quality.
Looking at the levels of obesity in the U.S., I consider the 26th place a true miracle of American medicine. If it can prevent people who devastate their bodies with junk food for decades from dying at 50 ...
On the other hand, imagine the world where Coca-Cola makes billions on healthy drinks, people are slim and fit until they die, and half of the money spent on treatment of chronic diseases of excess can be used for something else.
This is not unique to the US. Can't really say "but we only have 25% obesity here" and call that any kind of win. Maybe the US leads in this regards (though it varies by region, some areas have European-level obesity rates), but obesity is a worldwide problem.
>Medical decisions need to be made outside of cost considerations.
It's really jarring to read an otherwise reasonable comment that drops a whopper like this. Nothing exists outside of cost considerations. The NSA has cost considerations. The Space Shuttle had cost considerations (obviously, not great ones!). The design of nuclear submarines involves cost considerations, however unsettling that may seem. You're telling me that my broken hand needs to be judged outside of cost considerations? Give me a break.
The problem is that there is a lack of "trustworthy" parties to evaluate cost expectations in medicine. The patient often doesn't understand their condition or its treatments, the doctor has a clear perverse incentive to inflate costs, and the insurance company may actually be better off if the patient dies. At least that's the conventional picture. Leftist pundits often complain that the American economy is based on "greed", but a more precise criticism is that there has recently been a trend away from expecting benevolence and for-its-own-sake honesty from anyone under any circumstances, or equivalently an increasing cynicism about human motivations. It remains to be seen whether a medical system can function when nobody expects to trust anyone.
> * In stark contrast to asking questions and trying to understand. But I have family members who are the "look everything up and then try to tell my doctor how they're going to treat me" ilk and it's crazy.
I think this is exacerbated by doctors a lot of the time. I'm in Canada so it's obviously a very different system, but visits to a GP often have strict time limits and "one issue only" rules. When you can only talk about one symptom, and you only have 5 minutes to explain it, it's natural to try and do homework first to see what you're going to use your limited time on.
> * I strongly believe that only physicians should be running hospitals.
Strong disagree. This same attitude pervades the military ("only pilots should run the air force") and really all it does is that lower representation of the interests of the other non-pilot 90% of your organization and put a pilot bias on every decision being made.
Those are extremely different situations and you’ve not really justified why they’re being compared. A “doctor bias” in every decision being made would ideally prioritize health outcomes over decisions made for profit or convenience. It’s possible that doctors will make poor decisions too, but on balance our expectation based on their training is that decisions made because of healthcare outcomes would be more likely in this scenario than the current state of affairs, which prioritizes economic considerations as administrators in every context currently tend to
I think the point is that "doctor bias" will not take a balanced approach to the other systemic factors. I'd argue it's the same with the pilots. If you asked pilots, they'd likely say the same thing: their priorities are going to align with the mission better than anyone else's.
Anecdotally, this has been true in my experience on complex engineering projects. When the project manager is a mechanical engineer, guess which systems get the most time, money, and priority? Mechanical. And when it's an electrical engineer, the electrical system gets the priority. When it's a software engineer, the software etc. They all recognize the other systems, but availability bias skews their worldview and priorities to the neglect of others.
> I strongly believe that only physicians should be running hospitals.
More than that - hands on healthcare should not be a for profit industry. The need to make profit is fundamentally opposed to providing the best care. As the push for profit increases, more people get sick and die. This goes for long term care as well, which is facing a similar staffing crisis for similar reasons.
Your local hospital is likely a non-profit. Your health insurance company might even be a non-profit. But they don't do any better. Corporate profit motive doesn't seem to be at play here.
>I strongly believe that only physicians should be running hospitals.
Can you elaborate on your rationale? I ask because I've worked in hospitals run by a cadre of physicians and it was not run well. Anecdotal, obviously, so I'm curious on your thoughts on what they provide.
My worry is that it can lead to an unbalanced technocracy. It's like saying a politician needs to come from [industry x] to govern [industry x]. Technical competence is a necessary, but insufficient criteria when managing a multifaceted problem. The risk is that the front-line physician priorities would always become the organization's top priority. In reality, a hospital administrator has to manage competing priorities across many different domains.
> after service has been rendered can decide to pay less, or not pay at all, or stop paying that provider altogether, etc
This actually isn't necessarily true when you learn how billing codes work. Most insurance companies pay out at a fixed rate per billing code based on your plan. That doesn't change. What does change is that hospitals can retroactively apply new additional billing codes.
This happened to us once for an ER visit where we got 3 additional surprise bills over 6 months because the hospital retroactively applied new billing codes to our visit.
Opposite anecdote: For done reason about 10 years ago my asthma that had just been a minor nuisance and didn’t stop me from running, teaching fitness classes part time, etc. for a decade, sent me to the hospital and kept me coughing for nearly a year.
The doctors and specialists gave me every treatment under the son to no avail.
Then I did my own research and read I should try OTC psuedophredrine. It worked like a charm. Now every time I catch a cold (and when I got Covid), I pop psuedophredrine for a few days and I am good.
Yes, psuedophredrine is suggested to treat Covid if you have virus induced asthma.
Second anecdote: I have relatively mild cerebral palsy. As I’ve gotten older, my affected foot tightens up especially in the winter. My neurologist said it was physical and not neurological. I went on vacation and was drinking more alcohol than I usual do. I noticed I was walking without pain. I did my research when I got home and found a prescription muscle relaxant with the fewest side effects and ask my doctor about it. He prescribed it to me.
He didn’t bother telling me that I should get blood work done to check for liver problems. I had to bring it up to him.
I can now walk without pain and run when properly conditioned.
* In this day and age not being your own doctor/advocate will produce unwanted unnecessary results.
If you look up possible treatments /side effects and your personal history you will be in a better position to engage and weight options. If you blindly accept everything you will end up on the most profitable treatment plan plan insurance allowed.
>I strongly believe that only physicians should be running hospitals.
(Disclaimer: I have been on the design team for several hospitals, including El Camino and San Francisco General, in the bay area - and I have a family of doctors and nurses in my family - my brother was head of the Veteran Administration for the state of Alaska, and is currently CMO for a large health provider (he is a doctor)
---
That said, the "running" of a hospital isa hell of a lot more than medicine (when we are specifically talking to the running of -- but this comment was made in relation to costs/efficiencies as far as outcomes, patient treatment, insurance etc...)
Hospitals are really complex ecosystems and should be thought of more like an aircraft carrier than an other form of business.
The costs within the realm of a hospital are ridiculous - as are the methods and manner in which hospitals raise money.
Insurance is cancer to be sure, but there are so many other factors that go into the operational costs of a hospital - and I don't just mean ngoing care and operations - systems and technology and medicine evolve. People are people and regardless have the same hierachy of needs in any environment.
You have every single actor as an enemy of the hospital bottom line:
New tech, $$
Older nursing pop $$
Current nursing/doctor market salaries $$
Maintenance for existing systems $$
Insurance billing code lock-in $$
Competing hospitals for doctors and nursing staff $$
California $$
Corruption $$
Utilities and related redundant infra to ensure life systems
The ridiculous cost to upgrade
The list goes on and on...
(The cheapest hospital project I worked on was hundreds of millions of dollars)
etc...
Hospitals are really expensive to run, and it requires a hell of a lot more skills than simply being a "doctor" to run one.
Let me add two more payment scenarios:
1) Pay in the form of a credit card number, where the provider ends up paying CC processing fees to process the payment.
2) Ask for the money back, months later.
> Insurance is the only industry where they agree to pay for something (in this case, "medical care"), but then after service has been rendered can decide to pay less, or not pay at all, or stop paying that provider altogether
This is precisely why I think we will never be able to effectively treat healthcare as a "free market" with tools like HSAs, posted price sheet, etc. The end user can never know the true cost of their procedure until it's long over (sometimes years later) and often don't get to choose at all.
The hospitals themselves are also to blame. There are a couple court cases where the hospital threw the nurse under the bus to cover up for their own issues (short staffing, bad safety procedures, covering up for a doctor, etc), and nurses are justifiably pissed off right now.
There was a time when hospitals could have helped the nurses with the stress and workload, but the admins bungled it at every possible turn, and now it seems they missed their window.
Sample size of 1, but my gf blames forced overtime. Being legally obliged to stay for an 8 hours shift after finishing one has a way to drive you to depression.
I would pay more to go to a hospital where I know people are actually well rested. My last few hospital stays have been saturated with clearly agitated staff (doctors, nurses, reception) who were putting in minimal effort, and clearly didn't want to be there, and I can't blame them given the conditions that they're being forced to work under.
This is in the US, and I can't figure out why the Department of Labor hasn't cracked down on the medical industry yet. It's really horrific, especially because these are the people we're supposed to be relying on to keep us healthy and safe.
How hard is it to enforce 8 hour days 5 days a week? Every other industry has figured it out.
To be fair, most industries don't have evening and night shifts and a supply mismatch, most nurses want to work the day shift, it's harder to find candidates for evening and night.
That's a little bit different and not as detrimental though. It's actually an incentive for nurses because they get to work fewer days. Instead of doing 10 8 hours shift every two weeks they'll do 6 12 hours and basically get 8 days off every 2 weeks, which is pretty interesting from a free time perspective.
My gf did both and while she was tired after 12 hours, overall I think she preferred it.
Canada's solution will be to mass-import nurses from the third world who will do twice as much work for half as much money. Mark my words.
It's already happened with low-wage fast food jobs. Health care is next. Nurses and doctors will be replaced by poorly-trained third-world counterparts.
> Canada's solution will be to mass-import nurses from the third world
Yes that's basically what Quebec (and probably other provinces) is doing.
> Do twice as much work for half as much money
I might get tomatoes thrown at me for this, but anecdotally "third-world" nurses are usually not as good due to having experience on different equipment, drugs and often languages. It's better than having no one to cover the shift, but it can be seriously dangerous due to lack of training on specific protocols.
They get paid the exact same amount of money and are in the same union, so they absolutely don't do "twice as much work for half as much money".
I agree with your assessment regarding foreign trained nurses. I think it also applies to doctors as well.
Regarding the pay structure for nurses, over time the unions will be filled with mostly third-world ones, so I predict their bargaining position will be weakened and they will accept worse conditions.
Instead, you're left with the diminished quality of care from people who desperately want to leave but they're only there because they can't afford to.
In the book The innovator's prescription: a disruptive solution for health care by Clayton Christenson, there are some good analysis of where the complexity and problems come from in the current US medical system.
A lot of it has to do with size and the complexity that goes along with it. So, as hospitals get bigger, do more, and increase in size and complexity these issues become worse.
The economics math even mirrors factories... a factory that can build 100 things compared to one that just produces one thing.
The book was enlightening, even though many of the time frames called out in the book were wrong. Disrupting medicine is a lot harder than something like technology.
So like a 2000 bed hospital just for heart surgeries. Like you're saying, the more a heart surgeon specializes, the better they are at it and the cheaper they can do it. Better Outcomes for less money.
Yes there are hospitals in India that cater to a specific aliment. For instance, eye hospitals, cancer centres, hospitals that cater to pregnancy, childbirth and neonatology etc.
> Like you're saying, the more a heart surgeon specializes, the better they are at it and the cheaper they can do it. Better Outcomes for less money.
Not necessarily.
1. A heart surgeon is going to be doing heart surgery at more or less the same frequency regardless of whether the hospital they're at handles only heart patients or not. Wouldn't they?
2. I doubt if anybody here considers them cheap. Yes it's probably cheaper than in the US, but still it's rather expensive. But then again, since life is priceless, ...
At a 2000 bed facility though, you could specialize in specific types of heart surgeries. At a general hospital you're probably more likely to take on a wider variety of heart procedures. It's not just experience, but experience in specific procedures that can dictate outcomes:
I see your point about experience with a specific procedure. Makes sense.
About the cheapness aspect, what I've seen in India is that if a hospital specializes in a specific type of treatment, there's a good chance it is going to be expensive. Unless it's run by the government or something. But a lot of super-speciality hospitals near me are private hospitals.
It’s like that in many countries, also in EU. Average age of a nurse is rising, richer countries rescue themselves by importing workforce, because they can’t find workers for the rates they have budgeted at home.
It’s is like that in other professions too if it’s only the tech that gets compensated well. There is a shortage of skilled labour.
Errata: there's a shortage of skilled labour for these working conditions. Said budgeting is not set in stone, and as long nurses and whatever else professions can vote with their feet (by leaving the profession) no amount of politics-led finger-pointing can replace a real-world change in the healthcare policies.
There’s near-infinite demand for healthcare and a constrained (mostly artificially) supply.
Insurance, people and government can’t solve the problem of the supply and demand by throwing money on it.
You either expand supply or remove demand. Given removing demand is... not desirable. The only alternative to fix the issue is remove regulation and expand supply. That’s it.
Insurance makes the issue worse by increasing demand and in a way limiting supply through requirements and procedures.
Government limits supply through regulation AND expands demand by paying for procedures.
An approach is to deregulate, such as removing government licensing, remove Medicare, etc.
Imo Prices would drop >95% within a 2-5 years (to India or Mexico levels).
I worked in medical billing for a few years and the issues are beyond obvious.
I think there needs to be some new approach to how medical services are being paid for. My 70yo father fell off a ladder and drove himself to the hospital in Calhoun Georgia (2 hours north of Atlanta, a small town) with a bruised eye and a broken wrist. He got in late afternoon, left the next day, and the bill to insurance (which of course they won't pay) was $69,000... more than per capita income in the US. The system is ridiculous.
In my opinion, healthcare has reached the state where the people who receive the benefit are too far removed from the people who pay for it and given there is no "victim" of price gauging, the prices will just keep going up up and way.
I defer to those wiser than me for the solution. I don't like complaining without being constructive so here is my ignorant pass at it. This will require a few key steps: 1) Yes, we need more supply (by deregulating the profession) 2) I personally think a more effective solution would be to gradually eliminate insurance except for catastrophic risk (like emergency medical care from a car accident). #2 will shift responsibility to the individual and the system will be capped at what they can charge based on the average person's ability to pay for it (which is how it works in many parts of the world).
> left the next day, and the bill to insurance (which of course they won't pay) was $69,000
I agree with you and the quote above is because of insurance. Medicare will pay 10% of that total and your father would be charged 2-5%. If he has private insurance you’ll see something different, maybe 15% and your father would be charged 3-6%. If he’s going out of network could be 100%. Hospitals / practices charge insane bills because people pay just a small fraction typically. It really impacts those without insurance or private insurance the worst. It is insane.
This is why I have suggested deregulation, particularly around licensing. It drives down the cost. Insurance may cover doctor X, but if nurse Y can do it for 5% the price... well use the nurse. All doctors would have to reduce prices and insurance would have to raise the coverage amount to compete. It’s what is done elsewhere in the world.
I don't think it has to be binary. For situations that are life threatening, I'll opt for a premium service and for situations that are not, I may opt for an alternative. I think almost anyone at our company can be trained to reliably operate and interpret an x-ray machine for the vast majority of use cases.
'For situations that are life threatening, I'll opt for a premium service'
1 - what does the 'non-premium', i.e. bottomn of the barrel service look like, is that incompetent people offering rock bottom prices (resulting in death?).
2 - are you sure you can identify a life threatening situation correctly? Because my father did not.
3 - how do you know the 'premium' provider in question results in better outcomes, rather than being the same rubbish well presented in fancy packaging?
Re #1 and 3: you have this problem with or without my system (take a look at plastic surgery clinics in Miami for example). Doctors can be incompetent too and the system is so opaque you can’t readily identify or measure the outcome.
I think markets are efficient here and there are plenty of services we operate in now with similar spectrums of quality (food, airlines, general contracting, dental work, etc).
The gap between my position and yours i believe fundamentally is that I believe people can and ultimately should be accountable for their decisions. I suspect you believe they need to be protected by a system of accreditation. I guess I don’t put too much weight into that.
When you own the outcome, you are far more likely to do research, ask questions, compare etc.
2- I’m very sorry to hear that. I believe most people can most of the time. The more people are tasked with doing this, the more likely they will be to invest the time and effort to understand their health choices, seek counsel of others and potentially lead healthier lives.
I too am a bit scarred by the medical system. My sister was diagnosed with colon cancer at 33 and it was discovered “just in time” because she kept rejecting the quick diagnoses multiple doctors in Boston gave her. Had she not self advocated she’d likely be dead. I made a similar mistake when my son was born during Covid. We went into an nyc hospital foolishly thinking that if you are nice, quiet and well mannered you will be treated with respect. My wife went into labor alone in a waiting room where she was abandoned for hours despite us telling them how long she was already in labor and her ringing the help button numerous times. I wasn’t allowed until she went into the delivery room but she never made it there.
The lesson for me was clear
1- do your research
2- be prepared to self advocate
3- doctors are humans. Humans make mistake, they have limited and often flawed memories but unlike software development professionals, they do not have the benefit of being able to deploy state of the art systems, technologies and libraries
Happy to take this offline if you care to. My email is in the profile.
You should educate yourself about how most of the western world manages to have a functioning semi social health care system. US is broken because of this blind fantaic faith in free marketsderegulation simplifications.
The problem is a large swath of the population that believe in all earnestly that squeezing profit is some magical tool for a functioning economy.
Too bad US is so good at PR, this mind virus is wreaking havoc all over the world.
I would say that most western countries do have both public and private healthcare. I did have private insurance here in Spain and it's nothing like in the US, as far as I can tell. Service was excelent and I didn't felt everyone was stressed.
In france your public insurance allows you to walk in a private clinic or hospital too, as a relative did and they cover her post-cancer treatment better than in the public hospital (by her account at least).
So yeah, "free market deregulation" may be an oversimplification but you have a problem in the US that's also far more than just being for-profit. We have for-profit over here and it works.
And that includes private & public institution doing medical R&D and selling their products to the national health services and private clinics, like quite a bunch of spanish companies do, for example. I say this becase it weirdly pops as an argument when it's totally unrelated, and it may be only a tiny fraction of the total cost.
> You should educate yourself about how most of the western world manages to have a functioning semi social health care system. US is broken because of this blind fantaic faith in free markets deregulation simplifications
Most healthcare in the west is subsidized by the US. The US market is far more lucrative, so companies do R&D and make capital from the US. The US also subsidizes in terms of both military and energy almost every western country. Even then, Europe has a higher tax rate and on average is far poorer.
I’m well educated on this subject and worked in this area in the US and spent time in other countries. You have no idea what you’re taking about.
"The US also subsidizes in terms of .. energy almost every western country"
These claims are outrageous and totally unsubstantiated.
How does US subsidise energy of France or Japan?
"Most healthcare in the west is subsidized by the US."
"The US market is far more lucrative, so companies do R&D and make capital from the US. "
You are subsidising the companies, not my healthcare.
And they pay out this money in dividends to shareholders. I am sure they are very gratefull, maybe you should ask them for a rebate.
Stop subsidising them and overpaying - do you think healthcare costs in Europe will rise? If you do, I've got a wager.
> US is broken because of this blind fantaic faith in free markets deregulation simplifications.
The US is broken because we somehow believe that a highly regulated market is "free" as long as the government isn't paying for it. We literally have the worst of both worlds.
> "An approach is to deregulate, such as removing government licensing, remove Medicare, etc."
This worked so well for Rosemary Kennedy when she could be prescribed an ice pick lobotomy. And so well for Eben Byers when his doctor prescribed him radioactive water, and he drank so much his jaw rotted off. It works brilliantly for this woman[1] and her cheap Turkish dentist work leaving her in pain. And for, well all of this junk: https://en.wikipedia.org/wiki/List_of_unproven_and_disproven...
Deregulation is what we had when things were terrible. Regulation and licensing is what we use to block the most obvious junk 'treatments' and the worst con artists.
> "Given removing demand is... not desirable."
Removing demand is enormously desirable. Regulate the shit out of CocaCola, Marlboro, and all the other health destroying parasites and their advertising, tax them, rework town and city planning to remove driving as the primary transport in life and all the associated exhaust fumes, rework public schooling and rebuild trust in the government and medics so people aren't anti-health-advice on principle, rework employment so that employees have some rights and aren't stressed out all the time with no sick breaks. Rework medical access so people can see medical professionals, and sickness can be caught and treated early, which reduces demand on seeing much sicker people later.
> "Insurance makes the issue worse by increasing demand and in a way limiting supply through requirements and procedures."
Insurance makes the issue worse by driving up costs to patients and at the same time driving down pay to medical staff, by insurance taking as much as possible. Without insurance, supply and demand could remain the same, medical staff earn more, patients pay less, and services be more efficient with less time wasted fighting insurance companies and filling in insurance paperwork.
Insurance companies is a symptom of the REAL issue.
Unfortunately the American public hasn't figured out what the real issue is yet. They reason why they haven't is mostly because the Democrat party , Republican party, entertainment industry , the Main Stream Media, tech industry, and the the Commission on Presidential Debates (CPD) has them occupied with the symptoms of the REAL issue in order to keep them chasing their tails.
The REAL ISSUE why healthcare isn't getting fixed is because of Conflict of interest.The American public hasn't figured out that going to congress who is riddled with conflict of interest and who designed the existing system that we have in place and is benefiting from it, might not be the best idea to fix healthcare.
In fact the best thing to fix healthcare (and the other 99 problems)is to STFU about it and focus ONLY On reducing conflict of interest in congress. Until we reduce conflict of interest in congress nothing will be fixed.
The Democrat party ,republican party, CPD and MSM want you focused on everything but reducing conflict of interest in congress.
In order to fix healthcare and any of the other issues we must FIRST try to minimize conflict of interest by implementing the following as a start:
1. Term limits
2. Closing or reducing revolving doors between private and public sector.
3. No private campaigning contributions. Use tech to overcome the need of money.
4. Reform lobbying by doing away with the money aspect of it and utilizing technology to get your voice heard.
5. Pay congress members more and better benefits, but in return demand complete transparency from financial information to limitations in investments , NCA , and make pay and benefits tied to the general overall approval of congress by the American tax payers.
6.etc
Both party and the MSM solution to fix healthcare is the equivalent of going to the MOB and asking them to fix crime in your neighborhood which the MOB is benefiting from and is promoting. It just makes no sense to talk solutions with people riddled with conflict of interest.
You want to fix healthcare stop talking about healthcare and get the individual republicans and individual democrats to put their political ideology on hold and join forces to demand that their party ONLY focuses on reducing conflict of interest in congress.
I've worked with both, and by far hospitals are much, much worse actors.
Hospitals are legally enforced local monopolies (look up Certificates of Need). Meanwhile, you might have a dozen choices of insurance companies, but they all suck because they have to take what the hospital billing departments give them and take the blame or risk being dumped by the hospital.
> You can’t do anything unless it’s exactly how insurance wants and only for what insurance will pay.
This is the part that makes the whole experience so sadly ridiculous. Nobody could ever tell patients what something might cost and let them make choices, it was (and is) "Sign here to acknowledge you'll ultimately be responsible for all charges, no matter what they turn out to be." But the insurance company doesn't operate like that, they say "Want to be part of our network? Guess what, you have to ask us for permission or we just won't pay you."
We need to rip off the bandaid, as it were, and reboot the damn system. Pick one of any number of good examples from other modern industrialized nations that have functioning healthcare, and copy it. Yes, everything will be a zoo for a while. We'll survive, and maybe even come out the other side with a better system. And maybe some bankrupt insurance companies, let me find my handkerchief.
It is definetely a (big) part of the reason, but if it was the only one, things wouldn't be in a similarly terrible situation in other countries. Take the UK as an example which has a single-payer system, and morale is overall really low, too, and nursing isn't an enticing career. (On a side-note, the BBC show "This is going to hurt" is quite good and on topic)
Apart from administrators and insurers, I think a large problem is that the job has become substantially more difficult and technology intense, while support and pay hasn't kept pace. At the same time, liability is more serious these days, which I don't think is a bad thing, but certainly sucks for the workers who have to constantly justify themselves and can get crucified for mistakes.
It blows my mind that super long shifts are the norm for a job that's generally more exerting/stressful than your average 9-5. But it's a viscious cycle now because of the shortages of qualified staff.
Here in BC we have a full on crisis where family doctors are retiring at an alarming rate and not being replaced.
> Everything is controlled by insurance companies. You can’t do anything unless it’s exactly how insurance wants and only for what insurance will pay.
Framed that way, this sounds terrible. But... the truth is actual health care outcomes for insured patients in the USA are extremely good. This holds in comparison to other nations, when corrected for GDP and patient income, etc...
"Insurance companies" are, at least in the narrow sense, doing what we pay them to do really well.
They may or may not be making things easier for nurses, which is a different metric. But nurses aren't their customers, we are. And we're getting a fairly good[1] product.
[1] Albeit extremely expensive relative to other nations.
Offer to pay in cash and it is amazing how much better the customer service and general demeanour is from a medical office - it always blows me away. They must REALLY hate dealing all of the insurance BS.
I had not done an eye appointment in years and years because my vision is generally very good - I went in expecting to offer cash, negotiate, and generally play a bit of hardball. I was amazed when the front desk person IMMEDIATELY perked up, looked super happy, and started offering massive discounts before I even threw numbers out. The eye doctors as well were very enthusiastic.
This. I had a great doc until a few years back. Best doc I've ever had by a long ways. He'd spend a good amount of time with you, actually listen to your concerns and even bring up recent papers he'd seen on topics related to my health issues. A few years ago he decided to mostly get out of doctoring because he was tired of dealing with insurance companies. For a while he went to a retainer model ($2K/year up front, $250/visit) and cut the number of patients he was seeing down significantly. I can't say as I blame him.
I've heard the same thing from mental health counselors and therapists. In wealthier areas many will just stop accepting insurance entirely and make people pay out of pocket to avoid all the insurance paperwork and requirements (some insurers require specific diagnosis to continue paying for services). If an insurer decides to not pay you? good luck. Now you need to throw hours of unpaid labor at them to get money you're owed.
Unsurprisingly, this means many normal people can't afford a therapist and they're getting harder to find.
Granted, there's a niche for cash pay docs. Example being psychiatry - it's extremely hard to find a psychiatrist who takes insurance, even Medicare. The good ones are all cash pay...
I don't hear it talked about enough, but I think the biggest problem with insurance is that their profits are pinned to how much they spend on medical costs.
In theory, this sounds like a great way to make sure insurance companies aren't just taking unreasonable profits, and that they are spending money on medical care, not administration, keeping the business lean.
In _practice_, what it means is that profits are constrained by medical costs, so the insurance companies are literally incentivized to pay _more_ for medical services. Originally, insurance companies were supposed to be an intelligent negotiator on behalf of their customers. After all, their experts should know much more than a layperson every will.
But with the poisoned incentive to raise costs, customers are basically held hostage by a bag faith negotiator. Not bad faith as in malicious, but in terms of having an enormous conflict of interest.
In the very early nineties, insurance companies lured doctors in with promises of referral if they would just accept certain terms. Originally, this was to the benefit of the doctor -- more referrals. But only originally: once lock-in occurred, the insurance companies began to set their own terms. They couldn't have accomplished this without some greed on the part of many doctors early on.
Consolidation's a big part of it. The last decade has seen nearly all the small practices and offices in my city gobbled up by a couple of huge companies. With that comes the MBAs and the bureaucracy.
The healthcare in my area is like watching feudal lords rapidly claiming their territory. With central fortresses (hospitals) and outposts (smaller treatment centers).
Yes. Prior to insurance. Insurance is the reason prices aren't transparent; insurance companies demanded discounts, so providers raised their prices to then say "you're saving X from list". But not every company had the same bargaining power, and individuals had none, so the actual desirable price to offer couldn't be made broadly available. With a hidden price (so no shopping around), that is discounted at wildly different rates (so no meaningful way for third parties to track it), and a necessary service (so no just avoiding it), in a private for profit industry, of course it skyrockets.
Our options are either to mandate publicly available price lists that are adhered to and hope the market pushes things downwards, mandate prices, or socialize insurance (so that the sole representative of everyone can negotiate the price downwards using the leverage of the provider risking losing most if not all their clients). Or, you know, keep doing what we're doing which is working so well (/sarcasm).
It’s always astonishing how I can get a fully itemized vet bill right after a visit and pay for it. Meanwhile going to the hospital is like “well gee, let’s submit to insurance, see what they’ll pay, we’ll readjust prices and then come back to you in a few months.”
Months after my last real procedure in a hospital, even after the insurance was settled, I could not get them to tell me how much money I owed them. Even when I went in person and told them "I want to pay you all of the money right now" they just shrugged their shoulders and told me they didn't know how much I owed them.
They just sent me a bunch of small bills in the mail one at a time and had a text field online where I could blindly pay them without indicating whether or not I had completed my payments.
Fucking beats me (although this particular hospital seems to be very disorganized). I will never understand why anyone would make it difficult for me to give them money.
I ended up getting sent to collections for $40-50 for missing one of the bills. Never in my life have I not wanted to pay a bill, but god forbid any large organization just take my money and leave me alone.
More than that, I can get an estimate upfront, that in 100% of cases matches the bill unless they find something additional they need to do, which they'll inform me of and create a new total estimate for.
Of note, my vet insurance doesn't negotiate on my behalf; they just pay X% afterwards. The price the provider quotes for a given service is the price everyone gets (probably; some of the smaller vets might modify it if someone is low income and in need).
Insurance companies are awful and should not exist, sucking up a lot of doctor time, but when it comes to nursing, hospitals are particularly awful, cutting staffing levels to the bone in order to maximize profit. People die as a result, and nurses are burnt out.
My SO is a healthcare worker as well, she just graduated 2 years ago and has major regrets about her decision. She'd leave and try and do something else but she has mid 6 figure debt, to make things worse she was rear-ended her last year of school and has back issues that make it hard for her to handle the 12 hours shifts.
She's looking to switch jobs now and her first offer expected her to travel to locations deep in queens, manhattan and brooklyn, seeing on average 50 patients a day. She currently works at one of the largest hospital chains in NY and is now negotiating an offer from the other largest chain, initially she was told to not worry about salary and that they'd be able to match her previous offer, then HR called her and told her she had 1 and not 2 years of experience so the best offer they can offer her is lower than expected, she said she wouldn't be able to do it so the HR people went to check again to see what they can do and it turns out they called up the hospital that my SO works at now and checked their pay tiers and said they can only match the number that they were told. The new position was close to where we live so she considered taking it anyways but they just called her again and asked her if she'd be willing to travel to other locations multiple times a week to help fill in gaps (but weren't even able to tell her which locations before accepting the offer).
TLDR: don't let your friends and family go into healthcare
The shift to EMRs (more-or-less forced by the ACA) has been a huge quality-of-life loss for doctors. Tons of time spent on Epic or Cerner checking boxes and selecting drop-downs.
Turned a "trusted professional" advisory role into a keyboard role.
There are medical scribes who will do all that for the physician and for dog-shit wages. Usually these are medical school-wannabes so they can easily be tricked into working for minimum wage, and once they're suitably trained the physician just has to briefly scan the EMR for completeness and sign off on it.
> How doctors of all professions lost their professional agency to do-nothing administrators within a generation is quite puzzling and a bit terrifying to me.
I'm sure this is the top comment b/c we as developers have basically lost our professional agency to do do nothings roles like project manager/project owner/"business people". It's frustrating. I've been in the game a long time. It was way more fun when the web was still new and for the most part didn't care a whole lot about tech.
The financialization of every aspect of life, in this case with for-profit hospitals through multiple layers of insurance middle-men, the exodus you describe would seem one of the natural byproducts from miles away.
> How doctors of all professions lost their professional agency to do-nothing administrators within a generation is quite puzzling
The profit model of the U.S. healthcare industry might have something to do with it. The fact that hospitals are run like businesses and have shareholders is insane to me. I know other countries' healthcare systems got hit hard by the pandemic too, but it seems like the uniquely capitalist nature of healthcare in the U.S. sets it up to mistreat workers and cut corners for the benefit of administrators and executives.
It’s not just that, some hospitals are outsourcing everything disenfranchising the people that work there. And I mean everything from the doctors themselves to IT to the cleaning lady to the food workers and selling the buildings to lease them back. It’s the fleecing of America.
If they can't throw some medication with pharma kickbacks at you, they probably won't do much at all.
My 6 month old son was put on topical steroids for a small rash on his back and the doctors solution when this turned into a progressive issue was more and stronger topical steroids.
Eventually I learned about topical steroid withdrawal, and after a hellish withdrawal period, my son has no real skin conditions.
And yes, my son at ~1 year old was red and bleeding like that head to toe.
When I brought up steroid withdrawal I was rudely dismissed by multiple doctors including dermatologists.
Doctors currently have willful blinders on at a minimum, and some may be a true embodiment of evil. I hope the whole for profit medical system crashes and burns.
Steroids are so commonplace and old, I really doubt anyone was getting pharma kickbacks in the case of your son.
There's just a large range in quality amongst doctors. What you're calling "willful blinders" or "true embodiment of evil" is more likely just a failure to adapt out of a simple paradigm: {Inflammation}->{Treatment = steroids}. And a failure to recognize when that was causing a loop. Maybe they forgot about steroid withdrawal. In fact, as someone with quite an interest in pharmacology and some background as a paramedic, this is the first I've ever heard of it, and I love obscure medication issues.
As I mentioned in my comment I mentioned steroid withdrawal to many doctors when my son was literally only sleeping an hour or so a night from itching and I was dismissed out of hand.
If its not kickbacks, then its such a terrible arrogance as to be evil.
How can a dermatologist not know of my son's condition? Particularly seeing as steroids have been around for a while as you've mentioned. Even when I brought the idea to the dermatologist, after a bit of head nodding his solution was another two weeks of a yet stronger steroid to `calm it down`, and then to taper.
There's a nonprofit trying to get doctors to properly acknowledge the condition.
There's as I linked above about a million videos of people recovering from TSW as well.
There's even a study out of Autstralia that followed 10 children with what was called bad eczema, but after a withdrawal period every child at max had pruritis on elbows or knees.
If my job were skin, and topical steroids was one of the main things I used as a tool, how could I not know about these issues? You'd have to be such a hack that nobody would consider you a professional, yet the same dermatologist that offered yet another round of steroids had his office on the penthouse suite of a downtown building with a showcase displaying awards.
It may seem hyperbolic to you, but you didn't live through this like I did. You didn't see your young child in complete misery due to medical authorities you thought you could trust misguiding you. It's evil of some form.
I am a systems engineer and software developer, and I have worked on multiple healthcare related systems including one for a major hospital system.
I wish I had more access to nurses during the process. I was always told they were too busy. I just wanted to observe, as I do with any client I write systems for, and was denied. I can say that at least 2 other groups were working on the exact same project as I in the hospital system, and we "won". We all worked in isolation from one another, I discovered the others by accident.
The top of major healthcare systems is wasteful and full of "little kingdoms". The ideas that "AI is going to help" and "nurses need to feel heard" are basically incompatible. Throwing money at artificial brains is always to substitute real ones, and the concept itself is contradictory to employee development. Why train a bunch of nurses endlessly on a subject when you can train an AI once?
We're supposed to be improving & developing people's lives here, not improving a box. For centuries we've found new ways of thinking that have made us better at science and medicine. Computers could do that, but we're not using them to teach each other. We're using them to replace one another.
It may sound silly, but I've reached the point that the theory Dune puts forth seems right.
I'd say it's highly questionable that this can be achieved in a reasonable timeframe, if at all. And millions suffer from easily solvable software problems (no communication, no testing and ground research, greed, bad ux), while you chase some current CS buzzword of the year that would win the assignment (AI, blockchain now, chatbots, VR before).
I think we agree? If you're saying that software should be more "easy to use tool" or "craftsman tool" and less "use latest flashy tech concept to replace people", then yes.
A lot of us are saying we need to increase the pay of nurses, but we also believe that medical care is too expensive. So, where is all that money going? There are a lot of flippant answers but they never seem to lead anywhere actionable.
I am not sure, and I'm not saying this is the WHOLE problem (in fact I am confident it is not), but... in 2017 (first hit I got googling) 7.9% of all healthcare expenditure in the USA ($275 billion) went to insurance overhead, vs 2.8% in Canada.
But yeah, in general, this is a problem (healthcare in general, healthcare expenses, nurse job experience) where almost all other countries with similar wealth are doing so much better than us, it shouldn't be that mysterious to solve it, right? It's not like, who knows if it's even possible to do better! Like, we know it is... figuring out what the difference between them and us isn't trivial, but it should be easier than something there isn't a model for.
The most obvious difference would seem to be how insurance (and universal coverage thereof) is handled.
In France, 18% to 22% of the money given to our public insurance is used for administrative stuff, which i thought was a lot. Then I learned that 31% of what my company pays for my private insurance is used for administrative purpose. So either private companies are way less efficient than public service, or i should immediately buy shares from Swisslife and others.
One example is drug waste. Insulin for example is charged per vial to the patient but usually only a minimal fraction is actually used and the remainder is disposed of.
That also assumes there is no response bias. The linked article doesn't seem to go too deep on methods but the source is a content marketing piece for Hospital IQ, so I'd take it with a grain of salt.
Also my first thought when I saw n was 200, lots of surveys make mistakes in sample selection or question writing but it seems with the responses here and my own observations being close to nursing, the main point checks out. Lots of burn out and leaving the profession.
Agree, I'm definitely not making any statements as to whether or not the burnout is real. I just think that a lot times the assumptions we make when we apply statistical concepts (like standard error) to real world data don't hold up.
lol.. what kind of calculation is this?
n is 1 in this case, the survey was not repeated 200 times from which you derived 90% as the mean number of nurses quitting.
It's a normal approximation of the expected variance (in terms of standard deviation) in the estimate of the mean of the sum of 200 Bernoulli random variables. Each nurses' response is considered an observation of a Bernoulli distributed random variable, and we trying to determine the rate of that variable.
You are incorrect that "n is 1" since, by that logic one survey talking to 100,000 nurses would be the same as one talking to 3.
If you would like an alternate, more Bayesian formulation we can use the Beta distribution which is parameterized by alpha (numbers of 'yes') and beta (number of 'no').
This approach is a bit more intuitive than the Frequentist method since it answers the question "what do we believe to be the expected rate of nurses answering 'yes'"
In this case alpha=180 and beta=20, we'll include uniform prior of alpha_prior = 1, and beta_prior = 1
For Betas the posterior is defined quite nicely as:
Thank you for taking the time to explain your modelling. Unfortunately I will need to read more on this topic, because I do not understand the intuition behind the priors "uniform prior of alpha_prior = 1, and beta_prior = 1".
The way I would generally approach such a problem is by running monte carlo simulations. Assuming the true rate of nurses quitting is X, what is the chance that a random sample of 200 nurses has the expectation of quitting >= 90%. To get the lower bound of the confidence interval, I will run this simulation for several values of X, starting at say X=60%, increasing until I get >95% chance that a random sample of 200 nurses has E(quitting) > 90%. Do you think this approach makes sense ?
Simulations are fantastic, and often necessary for tricky statistics problems, however what you are describing is reinventing so much of the wheel using simulation that you are going to be spending multiple orders of magnitude extra computation to get an approximately correct solution. You also do have some conceptual errors in your plan.
For example
> Assuming the true rate of nurses quitting is X, what is the chance that a random sample of 200 nurses has the expectation of quitting >= 90%.
You have just described the Binomial distribution [0], which is probably the most elementary distribution you learn about when studying probability and statistics (even the Bernoulli is just a special case of it). There's no need to run simulations to answer this particular question.
There are also some fundamental misunderstandings with your approach:
> increasing until I get >95% chance that a random sample of 200 nurses has E(quitting) > 90%.
The probability of getting > 90% 'yes/quitting' (i.e. more than 180) if the true probability 'yes' is in fact 0.9 is only 0.46. You won't cross your threshold of 95% here until you reach X=0.933
If you wanted to construct the 95% CI from pure simulation, a better approach would be to sample 200 observations from a 0.9 Bernoulli random variable (just sample from a uniform, and check if it's less than 0.9), compute the mean of the samples, and repeat this 10,000 or so times. Then look at the empirical CDF [1] (fairly easy to implement in code) and look at the lower 2.5% and upper 2.5% values and you have your bounds (which will be the same as the ones I posted within some epsilon).
I do recommend, if you're seriously interested in understanding this, picking up a basic probability/stats book and work your way through it.
I wish there was some law requiring surveying companies to fully disclose their method of contact and compensation. I can absolutely see an employee looking to leave their job being more receptive to taking a survey. Those happy with their jobs are not as likely to respond to third-party entities like "Hospital IQ" contacting them. Maybe the survey company masked this survey as a "pre-screen" to finding new jobs! We will never know. The process of recruiting survey participants has GREAT implications on the results.
A family member just quit her nursing job because she refused to learn yet another system. She was great with patients but could not stand the computer systems she had to use.
I feel like quitting receiving healthcare when a provider switches their records systems or adds a new one and I have to input all the same shit yet again (what the fuck is even the point of digital medical records? They can't keep even the most basic info straight anyway!), so I can only imagine what that's like for the people who have to work with it daily.
Anecdotally - I have an acquaintance exiting the field of pediatric nursing. They worked in the ICU and with chronic conditions (cancer, heart disease, etc.).
The deaths were always hard when working with little kids - and there were a couple a month. But towards the end of COVID they were losing 4 kids PER WEEK (anecdote - I have no data other than listening to them vent) that this nurse firmly believed were avoidable had they received appropriate care.
What caused them to exit was how the hospital handled COVID: they postponed all elective surgeries. For these children, an elective surgery was anything where they "wouldn't die tomorrow" if the surgery wasn't done (somewhat of an oversimplification - but ballpark correct).
During that time hearts got worse, cancer progressed, bodies shut down until electives became emergencies... Success rates of surgeries dropped. And once restrictions started lifting the staff was underwater, they had a huge backlog of "electives" piled up on top of the normal ingress - kids were dying from waiting.
No surprise at all. A lot of unnecessary stress (yes, more than enough, even for a pandemic) and the top-down approach of the institutions really broke the trust of the public in many healthcare systems worldwide. I think the sentiment would be the same even if wages would be raised (and in many cases they have been).
Considering it was bothersome for both healthcare workers and the public, in my opinion the friction is more between the healthcare workers and management/government entities (& their policies) rather than "some patient bothered me" cases.
Not only are nurses talking about leaving the industry, in the "newbie programmer" groups I help mentor in, there is an alarming number of people who were considering going in to health care/nursing, who are now seriously reconsidering their options, or changing majors in college mid-way through to move into technology/programming.
I guess my point is, not only is the current healthcare labor market at stake, but hiring/pay/working conditions now are having upstream impacts on the labor pipeline of people coming into the market, or evaluating entering healthcare. Having recently gone to the ER with my toddler, I can tell you this is not an area you want the market going for lowest bidder when you do have to use healthcare services.
The entire medical profession is insane and intentionally geared towards inefficiency and difficulty.
They pride themselves in it being so hard instead of realizing that this is glaring problem that needs to be solved instead of nurtured.
This begins from medschool being prohibitively hard, to a lack of global licensing process, to doctors being on duty for 36+hrs when you cant legally drive a truck without stopping after 8hrs.
I’m going to offer a counter point, anecdotally of course. My daughter is in university right now. She’s a in pre-nursing. She says most of the people in her major this year switched to nursing from other majors during the pandemic because they saw it as the most economically viable major compared to their previous major. In a nutshell the pandemic scared people into being pragmatic about their degree plan.
So hospital administration will have a fresh crop of graduates, new to the system, to abuse. The cycle will continue unabated.
My wife is a nurse in the NHS. She actually saves people from cancer, or at least prolongs their lives. Her work is difficult, with huge responsibility. She gets a pay cut this year in real terms.
I make slight improvements to computer systems. In most of the jobs I've done, despite my best efforts to work for reasonably ethical companies, I've not been convinced I've made anyone's lives better. Yet my salary is 2-3 times hers.
I find it hard to believe there can't be a better way to arrange this kind of stuff.
It's an interesting problem, because we currently align economic 'productivity' and pay rather than social value and pay, which is efficient since we don't have to redistribute resources between industries or roles, and resource redistribution is a dirty word, at least in America. My wife is a doctor and I make significantly more than her working as an SRE, when her job is significantly more difficult (particularly emotionally) and time consuming than mine. She's paid relatively well on a societal scale, but I'd still call it a labor of love. If you're not in one of the high paid specialties, you don't do it for the money.
Even in the (US) medical system, pay/insurance reimbursement is based on the number of procedures you do, not how involved the treatment is. This is why surgeons get paid so much more.
Athletes and celebrities are paid because of economic productivity? It definitely seems like social value based on restricted supplies.
If there are lot of participants in a labor pool, naturally wages will be under constant pressure. The barriers to entry also play a role.
For those RN's quitting, they will simply be replaced by foreign workers. It's similar to how certain jobs no longer have locals in it anymore, instead relying on migrant workers. It's the reality in Singapore for instance and naturally creates an implicit caste system.
Now the markets have evolved/evolving where incumbent locals are no longer granted the same privileges they once enjoyed, somebody who does not have the luxury to consider alternatives will be the ones who fill the jobs, and get the blame when the descendants of local incumbents cannot make their way back.
This is sort of the system I am seeing emerging and it explains the anxiety of us vs them. In reality, the government, markets simply do not care for such superficiality. It seeks to accomodate those who are productive, not sit around waiting for higher powers to "fix". And as such, this dynamic ensures wages in certain industries stagnate, and it's especially true in markets with the characteristics I mentioned above: low barrier to entry and abundant supply of labor.
Not directly, but indirectly, this is one reason why bigger companies can pay more than small companies, more efficiencies, automations, and economies of scale means the output per employee is higher.
Greed is destabilizing society everywhere you look.
1. Hire more nurses to spread the load around
2. Pay existing nurses more
3. Incentivize people to get the technical training required to become a nurse.
"But what about my boss's 4th home?" I know. I am worried about that too. i pay 1500/mo to live there, and the costs will probably trickle down to me. we will have to figure something out.
"But we don't have the money! Who is going to pay for it?" Well. Then I guess the goose is cooked. We no longer have the resources to run a functioning society. I want you to think about that, and maybe think if we could get the funding from somewhere.
We are out of trained workers. The money diet our overlords put us on has officially starved us. Welcome to the 3rd world. Hope you saved up enough money for a ticket to Elysium.
Nobody wants to take out student loan debt anymore. If you are over 30, let me fill you in: cost of college has gotten even more insane than when we were in school.
we are seeing the same thing in our courts. Everyone is mad at the PDX DA for turning people loose all the time, but the secret is: there are not enough public defenders, and we can't hold people indefinitely without cause. There are literally not enough lawyers graduating from law school/graduated in the past to fill these spots.
Our society is falling apart and all anyone can talk about is how lazy the homeless are and obsess over what genitals people are born with.
"Well. Then I guess the goose is cooked. We no longer have the resources to run a functioning society. I want you to think about that, and maybe think if we could get the funding from somewhere."
Absolutely! Thanks, this made me laugh out loud. It's almost as if the people in charge of society don't have the same interests as the rest of us..
I have family members who work in health care here in Canada. The fact that their wages are subject to regulation (e.g., they are effectively getting a paycut this year with inflation), they realistically cannot strike to improve their working conditions (people will die), and that their work is very demanding (physical labour, emotional labour, shift work, constantly understaffed) makes this an unsurprising statistic from my anecdotal experience.
This isn't a problem that can be solved by an IT solution. Nurses have more patients assigned to them than what they can manage. They don't need another system of forms and workflows to fill out in addition to their overloaded plate. If anything, the solution is the opposite of an IT solution in that hospitals must hire more nurses and stop following the recommended lean-management staffing numbers provided by software.
Nurses have an extremely hard job. Before my wife died, she spent days to weeks at at time in hospitals over and over again. She went out of her way to show them kindness despite her suffering, and they always thanked her for it. Most patients treat them like slaves and are even abusive toward them- at the very least, thankless. COVID only made this worse. It's no wonder they are leaving in droves.
Agreed. This article is so off the mark, trying to talk all the ways technology can help this problem without a single sentence retrospecting about any of the problems that shitty EMRs have caused or at least facilitated. The massive increase in charting, and the fact that nurses spend more time on CYA than providing care these days is the number one reason I've heard from nurses who are trying to get out. High patient-to-staff ratios is the second, which wouldn't be quite as bad if it weren't for all the charting.
I've known a few nurses, doctors, and PTs who expressed exactly this sentiment. It's such a stupid problem, too. There's no reason they should have such an onerous burden, and yet they all do.
One of the PTs I know spent at least as much time filling out paperwork as he did with patients. This was partly due to the volume of paperwork required by govt / insurance / lawyers / whatever, and partly due to absolutely awful software.
Obviously the doctors should have done the paperwork and you shouldn’t have had to deal with that. But it seems like the root cause isn’t that doctors don’t want to do paperwork, it’s that the insurance is introducing too much paperwork.
My primary care doctor dropped me a few years back. He said his solo practice couldn't handle the paperwork of having so many patients so he went to just seeing patients for his specialty.
He was admittedly older and had never particularly embraced computers and so forth.
(And then my new PCP retired during the pandemic.)
In the 20 years since I've graduated college, the longest I've had the same PCP is 3 years, about half of the remainder I had for 2 years, and the rest I only saw once before they left and I had to change again. Even if they do stay, they have to see so many patients (~1000 per PCP is what I've heard) that they won't remember anything about me, and will be no better at treating me than a doctor pulled at random.
For people with chronic conditions a PCP makes sense, for the rest of us it is just another pointless loop you have to jump through.
almost every single general/primary care Medical Doctor's office in this area of California closed doors after the year 2000 or so.. Paperwork related to insurance billing, and inability to compete with Big Managed Care (Kaiser Health) for work conditions and benefits, is what I heard as reasons.. the offices were empty commercial space, it was noticeable how many there were...
Obvious bias, since I work there, but Elation Health is very focused on building EHR software that makes it possible for independent primary care providers to be successful and not have to spend hours per day doing paperwork.
Speaking from personal experience, moonlighting as a paramedic, paperwork is a universal challenge in healthcare (I often spend more time documenting a call than the call itself took from patient contact to transfer of care to the ER). It is shockingly rare for EHRs (regardless of the speciality they focus on) to actively try to make life better for the clinician. That's a large part of why I'm at Elation for my day job; the founders (and therefore the whole company) have a ton of empathy for the doctors (and staff) we serve.
He was part of a hospital system so he used their software. I know nothing about medical software but my impression is that there is a huge amount of paperwork regardless involving insurance, prescriptions, testing, etc. Stuff is more integrated and electronic than it used to be but there's still a lot of manual interactions, phone calls, faxes, etc.
My wife is a PA - here are a few things we've (anecdotally) noticed:
1. A few doctors left practices after they got taken over by a bigger entity and the hoops they had to jump trough weren't worth it, so they retired.
2. The insurance companies - they control EVERYTHING. One thing that happens a lot is that they don't allow her to order an MRI unless she orders an X-Ray first - even if what they're testing for wouldn't show up on an X-Ray. And this slows down the process of diagnosis by days. There are more examples of things like this - things that should be up to the provider, but end up being up to the insurance company (what drug to prescribe or what treatment to pursue first) - it makes no sense (at least from what I hear from her).
The software in this space is terrible. The system is designed for admins not practitioners. For example blood pressure entry is odd with two boxes. Note capture is slow due to needing it be typed rather than written. Sharing out of the core system is onerous.
FHIR would be a good idea, but in practice its hard to correlate a patient across the systems. Few hospitals and doctors setup a push notification for when they change a patient's record.
Essentially all of the software needs to be redone with a focus on a centralized record tracking system. The rewrite needs practitioners (all of them, not just Docs, but the lowly CNA too) to drive the requirements. Admins should be included, but not the target of day to day UI.
During my last physical, the doctor was trying to listen to my symptoms while getting frantically pinged from the hospital or something. I don't blame him at all, but this trend of always-on + interruptions at work is disastrous, I imagine especially so for people like doctors doing extremely high level intellectual work.
My partner is an NP, not only is there an astounding amount of paperwork, usually it's done outside of working hours because management took the chunks of the work day that were previously blocked off for doing paperwork and turned them into more patient visits so they could make more money.
this is more correct, the medical fields have to do a lot of paperwork to follow rules and avoid issues (legal?)
almost half of their time are on charting instead of taking care of patients, paperwork is needed, but in most facilities, it takes too much time, and the workflows are not optimized enough as well...
I've always wondered why they don't hire an assistant that JUST does the paperwork/coding for the doctor. They could follow them into room and just take notes (and leave at times when it is appropriate).
How much could it cost to pay someone else to do this? Surely less than a doctor makes doing it... It can become its own profession. It's a separate skill - separate from what a doctor should be focusing on.
On a side note, it seems that a lot of professions would benefit from having an assistant - a thing that seems to have disappeared - if what I've seen in old movies in shows is to be believed. Another side-case of this is the fact that technical people tend to be promoted into management roles and have to deal with attendance and time-sheets - why not have someone else do it? The work only suffers.
My kid's pediatrician has a guy that does this. The job title was "Scribe." A little bit crowded in the exam room but you get used to it.
The Scribe had a laptop and could look up whatever info was needed while the doc was doing his thing. If a scrip is needed the scribe types it in to the system and then the doc had to read it and approve.
Just keeping the docs hands clean from not having to touch a dirty laptop/iPad all the time has a health benefit I bet.
Brilliant suggestion.
Some of us still remember the days when we were paid to be creative engineers, solid creative engineers, designing elegant solutions. Didn't know or need to know how to type, design layout of reports, kerning and fonts, didn't keep track of bills and accounts:
Just engineering. (Of course report presentation, review and editing were still necessary, not not the actual technical aspects.)
If nurses could work a regular 40 hours a week and be paid more, as they would like, the additional money and staffing need to come from somewhere. In the United States, we've decided that private hospitals could have the right to exist. Most nurses are thus beholden to a free market. So the question is why other hospitals aren't trying to poach nurses with better wages and schedules. The reason may be that the supply of nurses remains large enough that hospitals don't feel pressured to make these concessions. The business model of hospitals is also drastically different from that of, e.g., tech companies. Tech companies can afford to pay their employees outrageous salaries because it is possible for one software engineer to create a product that will generate $100M in revenue. A nurse's labor has a cap on how much economic value it can generate. Hence why nursing salaries are constrained.
From such a high level, staffing may not seem like a problem. When it comes to the hospital floor level, staffing's been a big issue these last two years. Keep in mind that the common 12 hour shift for a nurse came about because of 70s staff shortages.
> U.S. nursing salaries relative to average U.S. wages are above the OECD ... So pay isn't the problem
Do you think when someone evaluates if they're paid enough they're thinking 'what is my income relative to what someone else's income is in Belgium relative to other people in Belgium?'
They do detail what the nurses themselves say are the problems in the article. I’m not sure I see a reason to doubt their reasons. They didn’t identify a shortage of doctors but rather a shortage of low skilled workers whose jobs they’re having to pick up in addition. Also while the population ratios might be in their favor, apparently the patient to nurse ratios aren’t. Even if they’re better than most of the world that doesn’t mean they’re necessarily happy - when you’re unhappy telling someone that there’s someone worse off doesn’t improve their situation.
Comparing the US with OECD isn't proof that pay or staffing aren't part of the problem. Nurses can be underpaid, and still earn more than their peers in other countries.
Also, it looks like the outrageous costs of healthcare in the US don't correlate at all with nurses' wages. If I were a nurse, I would feel demoralised if I was doing a lot of the hard work, yet administrators and middlemen still get the most money.
Most nurses work three 12 hour shifts and are paid for 40. It's so prevalent that a lot of them will pick up an extra shift or two at an entirely different hospital.
You don't have enough data to determine that as you are assuming that the staffing levels should be the same between countries when due to things like a huge push to increase profits, more paperwork, and other such things they can be drastically different.
It sounds like your last statistic means that U.S. nurses need to do more work than their counterparts in other countries (to make up for a lack of doctors), which suggests that pay and staffing might well be the problem...
These numbers don't necessarily tell the full story, since "nurse" isn't necessarily a fungible title across the OECD: nursing requirements and qualifications vary by country, as do the job's obligations. This is probably particularly true during the last two years, as nurses (everywhere, but particularly in areas that have refused vaccination) have assumed greater daily responsibilities.
There's even more in here beyond the headline about nurse satisfaction.
USA healthcare pretty broken, and sliding into catastrophe. Nurse dissatisfaction is just the tip of the iceberg, or the canary in the coalmine.
> Eighty-four percent of emergency room nurses and 96% of intensive care or critical care nurses have a 4:1 ratio, which is double the optimal target of 2:1.
> Thirty-six percent of nurses said they've seen patients with acute health conditions walk out of the ER because of the wait times for an inpatient bed. And 37% said that surgeries had to be rescheduled because of bed shortages.
I've worked in healthcare law for a few years and I think the problem boils down to how it's regulated.
It's super, duper complex with lots of paperwork. The complexity is too great to run a small practice, the Medicare/Medicaid fees are too small to make up for it, and it increases the importance of administrators in the hospital system.
If I had a bunch of time I'd love to go through and write up a proposed alternative approach, and congressional bill -- but I have to imagine even if I did that, no one would listen to it.
This isn't just a market failure or some inevitable 'iron law' of bureaucracy taking over management.
This is a society wide failure, and we're all complicit. Umpires, cashiers, pilots, referees, doctors, nurses, baristas, accountants, restaurant staff, bank tellers, flight attendants, and teachers are all quitting due to a belligerent, abusive, or violent public, uncaring administration or management, low pay, lacking benefits, unpaid work hours, or reassessed priorities. Little league and high school games don't need parents, players, or the coach smacking or screaming at the ump or ref. Nurses and even doctors don't need one thank-you basket/gift card for one employee per month, empty thank you slogans and parades, lean staffing/six sigma/JIT healthcare staffing bullshit, for-profit, private equity hospitals/clinics, pre-authorization and insurance managing healthcare instead of doctors, pay freezes, legally mandated pay caps, PTSD, or mental trauma from all this steaming pile of nonsense. Violence against medical professionals has gone underreported and grown dramatically over the past few years. Hospitals are allocating significant budget to security. In places where they've never had security. I'm not even going to touch upon all the myriad other issues right now. And, we're/they're not heroes. They're just doing their job, not saving the world as your personal, sacrificial lamb. It's just a job, not a heroic sacrifice. So yeah, we will all quit and play musical chairs with our jobs until things improve.
Hard profession but one of the last things to be automated imo, guaranteed income for next 30-40 years. Don't think you can say the same about certain types of doctors for instance.
A friend who is an anesthesiologist said that he was retiring because the new machines were so good that no one wanted to pay for an anesthesiologist anymore. They were happy with a nurse. So you're right.
CRNA != Nurse in the same sense as a registered nurse in an ICU or med-surge department.
CRNA is the Nurse Practitioner version of Anesthesiologists.
They're paying for less anesthesiologists and hiring more Certified Registered Nurse Anesthetist because they're cheaper, perform a sweeping majority of the same function, and multiple can be supervised by an anesthesiologist who is on hand to fill the small gap between theirs and the CRNA scope of practice.
It is very algorithmic in nature afaik, so quite easy to automate. As is oncology, radiology and many aspects of family medicine.
It won't be tomorrow, but 10-20 years from now I think is very realistic for huge changes.
Brave new world...
Nurses do a lot of menial tasks that they are overqualified for. Could those not be freed up by automation so that nurses can do the high-skill tasks they are uniquely qualified to do?
I think you're right in the sense that I expect we won't shoot to automate the menial tasks first, and instead will let our hubris guide us to automate the high-skill tasks. But speaking optimistically, there's a lot of productive automation that can happen. Heck, a lot of it has already happened via digital record keeping.
But much of those menial tasks are quite difficult to automate - changing IVs, bed sheets, patient clothes, bandages, diapers etc etc...I don't think AI/robotics is anywhere close.
However, it is possible that much of the menial work will be delegated to lower paid "nurse aides" that don't really need much medical knowledge , while the real therapeutic work start being automated by machines and algorithms.
Thus salaries will be squeezed downwards, which in the end is what the system wants obviously.
From my friends anecdotal experience, burnout in medical industry is partly due to too much administrative work.
It is also partly because the number of patients is increasing disproportionately, mostly because people are getting older. An individual at the age of 50 needed fewer medical appointments than an individual at the age of 70. That's literally from 2002 to today.
There just aren't enough nurses and doctors to tend to such a large old population.
My sister is a RN training to be a NP. Caring for others has always been in her blood. But I can tell she's not happy over the last few years (even prior to covid).
This survey has such a low number of responses to make any meaningful conclusion from. 200 people surveyed. Non surprising stats like 71% of respondents having 15+ years of experience wanting to quit.
What really should be the lesson here is that capitalism does what capitalism does best:
It cuts costs.
- More patients to nurse ratio (Simply unsafe given most medical professionals already lack sleep)
- Little to no compensation relief on the way. (Huge boom of travel nursing during pandemic)
- Excess job responsibilities (More paperwork/aid duties, less actual nursing)
- New talent / old talent challenges (Larger incentive to switch jobs, hard to properly train)
We better figure out something soon. The medical field feels like it's holding on by a thread. Insurance companies run rampant with no end in sight. Health care continues to increase in costs and fail patients to the point of walking out or even dying to get care.
While I think generally speaking, nurses like my sister just want to feel appreciated like other jobs people are burning out in. You can do that in many different ways:
- Don't overwork them.
- Don't underpay them.
- Don't give them unwanted responsibilities.
- Most importantly, listen to them.
I think you may find that people actually do love the profession as it's one of the most noble professions out there, just that they are being forced out of doing something they love because of greed. Greed is not good.
This is the direct and extremely unalterable consequence of one decision, to base our medical system on profit, instead of results, or capabilities. We've left a matter of national security in the hands of rent seekers.
The tragic insertion of a middle layer, the insurance industry (AKA Death Panels), makes it even more tragic and inefficient.
You can not seek profits in a competitive environment without reducing every cost to the bare minimum. Of course they are going to cut staff costs, and the number of properly staffed beds to the bare minimum, it minimizes costs. If a surge happens, they're happy to pay a little bit of a premium in the cost side for extra staffing. It's more than compensated by the extra billing.
But the recent public health emergency was a seiche, a tsunami, a pulse of unanticipated magnitude. (Unanticipated in the minds of those looking to meet this quarter's numbers, not in the minds of long term strategic thinkers).
The wrong type of people are in charge of health care in the US, and our nation will not be secure until this changes.
A good friend of mine was a nurse practitioner in cancer care here for 17 years, and quit last year to do contract work in interesting places. She's unmarried, no kids, etc., so I think it's a little bit of a "shake things up" thing but also a little bit "make hay while the sun shines."
Her most recent gig was in Antarctica. I mean, cool, right?
I would love to spend a winter at the south pole station. The biggest downside of being able to do my job remotely means I'll never get sent to cool places. :(
Looks like this is just the second time they ran this survey since 2018 [0]; there's no information in that one on how many were considering leaving (maybe 2021 was the first year they asked the question?) It always frustrates me when these stats are given without any context, how do we know if this is even high when we have no relative basis to compare? I think "considering leaving" is particularly difficult because if you were to ask me how many of my co-workers have told me they're considering leaving over the last year, my response would be near 100%. Yet here we are with only a few actually having left.
And why is it so hard to find the raw data from the actual survey? I'm surprised this is scoring so well on HN.
Poor pay, shift work, bad working conditions and multiple chances of catching all kinds of diseases.
Most nurses I know have above average intelligence with an excellent work ethic. Just one bootcamp away from a much better life.
So much sacrifice for the greater good, we the public are not worth it.
Another profession I always think of are math teachers, they are good people.
A bootcamp doesn't guarantee anything; without the right aptitude and temperament the tech industry is just as miserable, with a side of failure if you can't keep your jobs.
Of course a bootcamp does not guarantee anything and I’m sure the bulk running are probably trash. But I’ve met a few good engineers that originally were in other industry (HR, law, teaching, fishing) and they actually learnt the bulk of their software knowledge via bootcamps, so it can work. A good mentor is probably worth more in the long run but they are rare and not available to buy.
While some parts of the tech industry are miserable, on average they are definitely overpaid as compared to nurses or even doctors in some countries. And there are plenty of non miserable places in tech, especially if you relocate. Some Europe software shops seem out of this world when compared to US gaming companies, some of which sound like sweat shops.
As a physician, I can see that the 'corporatization' of healthcare has been a bad thing for patients. Unlike most other services whose use is discretionary, people do not choose to get sick. Healthcare is more like a police, fire or a disaster service. To allow a profit driven structure to use competition among providers to deliver this service will only harm the sick.
In the same way that national defense has been driven into a profit making venture (and encouraging the support for proxy wars), health care has become a beast beyond monopolistic power, able to drive demand for its own supply. The net result has been to give responsibility without authority to the providers. Nurses are subject to mandatory overtime. Physicians are required to take unreimbursed call. These services were once the hallmark of a devoted provider. Now they are exploited by a corporate profit seeking behemoth.
Patients now have such large deductibles that they prefer to pay me in cash for a negotiated lower price. No longer is health insurance actually insurance. It has become more of a coupon or in the language of today's generation, a groupon.
Even retirees who with Medicare only had to pay 20% of unreimbursed allowable expenses, have increasing burdens. The premium for part B (yes you have to pay for the part of Medicare that does not cover the hospital) has increased 15% this year and the government stated this is largely the result of a single dementia therapy - a pill that costs $56,000.
I think we could fix the problem if we required our lawmakers to actually pay for their healthcare. They get it for free. In addition, each gets a multimillion dollar stipend to run their office, separate and apart from their generous salary. For doing what? pushing emails. And they are so afraid of offending any part of their constituency that they spend most of their time arguing about non-issues. Their ridiculous behavior is creating a fertile environment for the next tyrant who will prromise salvation and deliver true misery.
at some point, somehow, medical care stopped revolving about 'healing' and medicine became all about 'treating'.
the health of the patient became subordinate to the economic incentives of the hospitals and the other involved institutions (insurance providers, pharmaceutical corporations, etc...)
and so I have the hypothesis that this happened because people (young adults) going into medicine because of a vocation to help and heal others become disheartened when they find out it's all about institutional profit; only them who get into this becuase "doctors make good money" really make it to the end (which is not terrible, as they usually do learn the methods and techniques of medicine, but that in the long run prioritize money over health).
health care should have never been allowed to become a capitalist marketplace.
I have a nurse friend that was fired because she did not want to take the vaccine. She had covid before, and strongly believes in bodily autonomy. She did not want to be forced to put something in her body against her will. She's started a business cleaning houses now, and says is making same money. Except now she
isn't pressured to be rushing from patient to patient like crazy. She's choosing her hours, works during the day at her pace and doesn't bring home the emotional stress of dying people. She worked as a nurse for 7 years and in that time she had thousands of patients. She said in all that time she only discharged 3 patients after chemo therapy. She's kind of convinced both are billion dollar scams by medical industry.
I work in healthcare but not as a nurse. I'm in a somewhat obscure field that became pretty important during the pandemic (infection control). No one outside the hospital knew we existed before the pandemic. Then the pandemic hit, conspiracies' started to float around and we had to take our contact list off the public website as colleagues were receiving death threats.
I can't even imagine what nurses have gone through being front line staff interacting with patients (and their families) all day. We need a zero-tolerance policy for families that verbally abuse front line staff, but instead they are often let off due to "stress of a family member in hospital" or the need for "family centered care".
As a patient I dread interacting with healthcare... but I can only imagine how horrible it would be to be on the clinical staff where you are wedged between people needing care and 52 bosses trying to minimize risk, maximize billing, and reduce expenses.
This seems like a world-wide pattern, and it was already an issue even before covid.[1] I'm curious about what alternatives they have, may be joining newer tech-enabled companies with nursing services, or going fully independent and work solely by their own terms with some patreon-like app... ?? Or is it the case that they are really sick of nursing and might prefer changing professions or even unemployment?
I'm a software engineer. My wife is a RN. It's been interesting over the past 20+ years to see the parallels in two different markets. Temporary staffing is used to fill vacant reqs. Gradual erosion of employer provided benefits.
Lots of blame being placed onto the business managerial class that has turned hospitals and the practice of medicine into a nightmare a la Kafka, but I think that the casual brutality of the healthcare educational model deserves a ton of the blame for this burnout. The reaction to all emotional trauma is to bury it and place all the energy into negotiating for higher pay. Money cannot endlessly sit in the place of enduring suffering, and the professions (medicine, nursing, PA, etc) will continue to degrade in quality as long as this barbaric understanding of emotional health is encouraged in the educational institutions.
High stress environment, stagnant wages unless you're a travel nurse, underappreciated during the pandemic, and having friends turn on you because they associate you with some crazy conspiracy theory. These are all reasons I've heard of career nurses quitting and going into other industries.
Conflicts with patients and their families. Politicians claiming you are overpaid and your friends and family believing them. Increased responsibilities without increased pay, something experienced nurses really feel.
I'm trying to think of how any of those can be solved with "technology" :-/
Nurses are paid well compared to the average worker in the US, but not compared to the service they provide. My wife, an RN BSN, was hit with a pay cut due to hospital system being bought out by another larger one. That's right, a pay cut, during a pandemic. Now on a fixed pay scale, with no raises built in. $3/hr shift differential for working night shift in no way makes up for the strain it puts on your body, your free time, and your relationships. Tons of attrition in her hospital and department, no signs of retention bonuses or anything other than a "We <3 our healthcare heroes" sign out front.
They're paid alright (generally speaking), but most devs wouldn't even consider a job at that rate. And the bar for entry is way higher: years of competitive and expensive schooling.
And that's ignoring the other factors that GP mentioned. I don't get assaulted on a daily/weekly basis. I'm not getting coughed on by COVID-infected patients who want to kill me because they don't believe that COVID is real. I don't endure a regular drumbeat of patient deaths and the constant second-guessing "what if I did X differently". I don't need to handle people's bodily fluids. And then there's the politics, internal and external (the conspiracy nuts, the fucked-up pecking order in hospitals, unions, insurance- and pharma-driven policies, politicization of healthcare, etc). I could go on and on, and I only know one nurse personally.
Nurses are not paid anywhere near "pretty well." They're treated like shit and the pay isn't anywhere near fair compensation for the service that they provide.
It makes zero sense for a person to consider straight-up nursing as a career in this age. The school is too competitive to get into, the pay isn't worth it, the job at the end is laborious, the culture is vile. If one does go into nursing, becoming an NP, CNA, or travel nurse are the only logical options from a time invested to income and burnout standpoint.
If a student wants a health care professional job, medicine and dentistry are better options and require just as much academic competition. Failing that, the student is better off going into tech or law.
If they're not smart enough for either of those? I dunno? Onlyfans? Permanent serfdom? I fear that our new society will have many who are left behind and struggling.
>but most devs wouldn't even consider a job at that rate
Lots of people ... most people work jobs that fall into that category.
I'm not sure that means much. I don't know how many folks who go into nursing are likely to just chose to be a developer or if it is that simple for them.
I know a few folks who went to university planning to continue on to med school, but ended up as devs for various reasons. Also, a vast majority of the audience for this site are devs.
Nurses are paid well, relative to the average American salary. I don't think they're paid particularly well relative to the job's lifestyle requirements and latent stress levels, especially during a pandemic.
Looking at my area (NYC), I'd have to take over a 50% pay cut from my engineering job to be "paid well" as a nurse. And I suspect my job is a lot less stressful.
While I don't doubt that nurses have very high stress jobs, the reason why you'd take a pay cut to become an nurse is because their job is a lot less technically difficult.
I have some friends from university who became nurses, one of which I was roommates with for two years during school. I helped them study for 'their most difficult math test' and it was a relatively straightforward test on changing units. They would not have passed a first year calculus class. The majority of their academic work was memorization, and then lots of hands on work in hospitals. The reason they get paid well is because the job is important and stressful, not because it requires highly technical people of which there is limited supply.
I don't say that as a slight - I know many nurses who are very intelligent people, its merely a judgement as to the academic rigor involved in getting your nursing credentials.
PS I worked at home depot during busy periods in the summer when the store was understaffed, I've worked as a waiter where I was the only person on shift because the owners/manager were idiots, and I've worked cleaning big chicken barns out in preparation for new chickens and those were all significantly more stressful than my technical work. Stress is not correlated with difficulty or limit of supply.
Were your friends NPs, CNAs, or something else? There's a wide variety in nursing roles, with a corresponding wide range in technical difficulty and expected proficiency. The average NP is certainly more technically proficient than the average undergraduate with a CS degree, albeit not in a domain the CS undergraduate might understand.
Tangentially: I'm not sure what the relevancy of "passing a first year calculus class" is. Just about every BA/BS passes one, and I (a program analysis researcher) have never even remotely needed by calculus knowledge in my day job. I don't think it's a good proxy for technical skill whatsoever, given that "technical skill" is a domain-specific qualifier.
I think the "hardest" job I ever worked was a PC tech support call center or a job at a pizza place. I didn't pick my hours ... and the job was a heck of a lot harder than my coding job that pays WAY more.
But it wasn't like I could just go and get a coding job at the drop of a hat.
Sure. Both programming and nursing are relatively niche fields. Nursing is arguably a significantly more professional field, given that (1) formal requirements are higher, and (2) Nurse Practitioners are effectively educated at the MS level (versus a BS or lower for the average programmer).
If we're using job difficulty and stress as some of our metrics for fair pay, then I would argue that tech support and pizza delivery should also be higher paying! But even with that, it doesn't seem unreasonable to factor in the professional qualifications (and corresponding time and money commitments) required of nursing. Relative to all three, it's a remarkably low-paying job.
I went to an undergraduate school with a fairly large nursing program, and interacted with a fair number of nursing students. One thing I noted was that a large proportion of nursing students were first-generation college students from lower-middle-class and working class backgrounds. I suspect that the meme of nursing being "well paid" stems from the fact that it is a step-up in that context.
This is my antidotal experience as well from extended family and friends. Many (mostly young women) weren't really sure what to do and picked nursing because "it pays well" and had a romanticized/simplistic view of nursing. Didn't seem particularly interested or passionate about it, so I can see how many would lose interest once the reality of the hard work in the midst of a pandemic.
I don't think they are paid as well as they should be considering the need for most nurses now to be on-call 24/7 and dealing with the stress from patients and their families, and administrative bloat.
It depends on where you go (and when; things have changed somewhat recently) but I know some CNAs who never became RNs because the time it would have taken to claw back the money spent on the degree wasn't worth the added stress of actually being an RN.
My mom was a RN (Registered Nurse) for 30+ years. She quit doing what most people think of as "being a nurse" about 10-15 years ago and switched to related work (home checkups, teaching, medical billing, etc.) because of how stressful and demanding working the floor in a hospital was.
Last year she retired from the profession entirely, a few years ahead of "normal retirement age", and now she works part-time at a local farm/fruit stand. The main things that drove her to retire early was management insisting on 12 hour shifts and not hiring enough staff.
Yes, you're right, and there are some reasonable arguments for it. But I'm not convinced that it's the optimal solution for all situations.
I my mom's case, she was mostly doing paperwork, so many of the arguments weren't as applicable. She had done 8 or 10 hour shifts for a while and found that she really preferred it (and was staying on top of her work), but then a different manager was brought in that forced everyone back onto the "standard" 12 hour shifts.
My last experience in a hospital was Dec'21. ICU, at an old friend's bedside, in a large (500+ beds, "teaching") hospital that is part of a big (50+ hospitals) chain.
The nurses seemed excellent...but the amount of time and emotional energy they had to put into dealing with multiple computerized systems - just within my friend's room, to replace an empty IV bag - was staggering. The "smart" IV pump was the worst - a crappy little display, a minimized number of flaky buttons as the only interface, and the nurse had to drill down into multiple sub-sub-sub menu's to do even basic stuff.
My first thought was that you could triple nurse productivity (as in "care given to sick humans") if you had two IT tech's following each nurse around, tasked with doing all the "re-redundant data entry & dealing with computerized shit" that had obviously become the nurse's primary job.
My second thought was that interfaces which the nurse had to deal with should be restricted to 1950's-industrial-control-panel style - nothing but well-labeled, single-purpose physical buttons, switches, & dials. And the data entry that they had to do was restricted to wax pencils on well-laminated paper - which could be fed to a scanner, to update the patient records database. (Displays, say of vital signs & such, could be fancy. But the "50's control panel" rule could put an end to "oh, that information is hidden down in a sub-sub-sub-menu here..." shit.)
My mom is a nurse and although she doesn't live in the US she also suffers from the same poor conditions. She has to work on the databases herself, staff shortage is a big problem (sometimes getting to 4 nurses in her "sector"). She gets underpaid even though she works 8 but usually 12 hours shifts sometimes in consecutive days (she usually gets paid 400 dollars per month if I estimated correctly). It's quite miserable but at least she a number of vacation days which she can choose when to "validate" them.
Get ready for another dark age. The destruction of education and medicine in this country means plague doctors will be making a return. Better check with your HMO to make sure your policy covers them.
A lot of the work nurses and doctors have had to do over the past few years has been truly soul crushing. Imagine getting a patient you know is likely to die and telling them that no, they can’t die at home. No, they can’t see their family. No, they can’t opt out of the then. For certain groups of patients, the work of nurses has turned into death row prison wardens, because there is a 10% chance they might be saved, and for a while there was no way to opt out of that.
Might be similar for teachers...I know many have cut back hours to part time where they can or are considering leaving. They are having to fill in for staff absenses and are stressed.
Anecdotally, many of my partner's coworkers have been on the school setting therapist -> hospital setting therapist -> burnt out craft store employee pipeline over the last couple of years, and my partner is desperate to join them once we have enough savings to allow her to quit her job. This is within the Speech/Language, Physical, and Occupational Therapist realm, so not nurses exactly, but it's similarly bad for a lot of medical-adjacent jobs right now.
"... poor processes, along with inefficient operational workflows and administrative burden are key drivers of frustration and burnout among ..." [insert job here]
This is pretty much universal in my experience. As a dev, it always seems to boil down to these. It's amazing how the business doesn't know their processes, can't document them accurately, or simply don't care to analyze and document them. Garbage requirements become a garbage system.
My mom is a nurse and although she doesn't live in the US she also suffers from the same poor conditions. She has to work on the database herself, staff shortage is a big problem (sometimes getting to 4 nurses in her "sector"). She gets underpaid even though she works 12 hours shifts sometimes in consecutive days (she usually gets paid 400 dollars per month if I estimated correctly). It's quite miserable.
What I've seen: health insurance companies and large medical companies were able to get everything they wanted. The result was Obamacare. It's been down hill from there.
I have family members in medicine, and they see the same thing. There was a really good opportunity at that time to address some glaring issues with healthcare, and we ended up with this thing that did not address those issues and created a lot more issues.
It’s a lot easier to say you will leave your profession than to actually do it, so I don’t expect anywhere near 90% to be true. But it won’t take that many to leave before it becomes a severe problem. The industry will be forced to reckon with this. We can’t not have nurses and healthcare is basically an infinitely large industry (people will spend all of their money to stay alive) so I’m sure it will be improved.
You see these numbers come out of nursing and teaching regularly. But they both have very high retention rates. Because in both cases, people stay because they would feel bad if they left. They're not there for the money. This is why they're so badly paid. This is why I didn't go into teaching: you cannot compete with people who will work for emotional rewards instead of cash.
My wife worked bedside at a nationally ranked childrens hospital for 5+ years. She left recently for private practice and loves it. More money, less stress, better management. The list goes on. Bedside nurses are often not paid very well, are treated poorly by patients, and even more poorly by administrators. The hospital’s motto should be “anything for the patient, nothing for our employees”.
My wife is a NICU nurse at a major NICU... she has worked there four years and is almost at her maximum pay, outside of COL increases, so right now she makes around $64k a year before tax/etc..
The travel nurses make significantly more and now that she has basically hit her cap (after just four years) I've been trying to convince her to move to a different unit or get a different job
We talk about insurance killing the medical field, but I'd also argue that EMR companies are doing a number on the profession as well. Have you seen the Epic campus? Epic - located in Wisconsin (not the gaming company). The amount of overhead a hospital needs to support/run that behemoth can't be small. And Epic is _swimming_ in cash.
Nurses is a tough profession. They are required to work for longer hours and not paid that much. With Covid, dealing with anti-science patients must have been very draining mentally. On top of changing the working conditions and increasing pay, may be we should make the nurses training free to make the field more attractive.
My wife works as a floater pharmacist in retail, can confirm, the situation is quite similar and very dire. She cannot even get a couple of days of UNPAID time-off when needed. The scheduler and the management are quite abusive with the way how they treat their staff. There is no such thing as a work-life balance.
Things will only change if nurses do more than just considering. Management don’t care as long as they have just enough nurses to get things done. Nurses are routinely sacrificed on the alter of higher profits and CEO bonuses. Only real action has any chance of changing the status quo.
If there ever was a contrarian move then it'd be for an 18-year-old to start nurse training now. Probably one of the last professions at all to be hit by automation, practically guaranteed demand for skilled labour and a hefty shortage thereof in the making.
It would be interesting to see data on this by state. Nursing, unfortunately, is much more difficult in states without unions. In California, the strong nurses union has ensured somewhat better staffing ratios and much better pay than in other states.
They surveyed "more than 200 hospital registered nurses based in the U.S.". Does this small of a sample size truly reflect the feelings of the ~2.4 million (2019) registered RN's in the US?
I'm so excited about the idea of creating an anarchic healing network of former medical industry workers looking to create a new system oriented toward meeting all the needs, not just some & also not for profit.
There has long been an immigration program for foreign doctors to gain the right to live and work in the US in exchange for first living in a rural/poor part of the US where most doctors do not want to live.
If have a nursing degree it's easy to immigrate to USA, in fact you will be coming in with a green card unlike tech worker. So to your point, US does prioritize nurses over others. Doctors are different and it's incredibly difficult for a doctor with a foreign degree to practice in US. I know this for a fact since I come a place where almost every other house has a nurse working in Europe/US
How are more people not sounding alarms about the future of our society with more bleak headlines like this? I fear we have become far too reactive to many problems that should have been anticipated, and planned for.
Nurses leaving the field is only part of the larger problem.
Nursing educators aren't exactly a dime a dozen. The average age of a masters prepared nursing educator in the us ranges between 56-62. Doctorally prepared is higher. The country is facing a nursing shortage, and a nursing educator shortage.
Now my doctor has an interesting theory that some of the pain points for nurses is being created by the hospital systems and industry themselves as an excuse to say we dont have enough nurses and bring in nurses from other countries like the Philippines, as they'll be glad to come to the US and work for less, and will be so grateful for the opportunity that they'll go along with whatever the hospital says they need to do. (This was in the context of vaccines.)
Many people in many professions have the same considerations about leaving. But then they realise they have a mortgage to pay, responsibilities (debts) they have signed up for, and never leave. Such is the system.
In Finland healthcare workers are striking right now, and instead of giving them the few percent raise they are asking for, the government is preparing a law to make it illegal for them to strike.
They'll leave with the teachers. Female-coded professions being derided for political capital as often as "inner-city crime" might tempt one to wonder which came first, the female-coding or the disrespect.
Just kidding. Teachers used to almost all be male until public schooling and the resultant budgeting turned them female (to pay them less.) It's like reverse computer-programming where the profession turned male when they started paying more.
Pay them and they won't leave. Pay them a lot, and dudes will start writing essays about how the reason women aren't being hired and are leaving the profession is because they naturally have less of an interest and aptitude for nursing than males.
There's no need to politicize this off completely unrelated tangent. The whole industry is under stress. It won't change. They will just hire foreign workers to deal with shortages.
Sometimes the only way to recognize and solve problems is to go through a crisis. I hope all of these nurses quit and the rest of us wise up to how important they are.
Meaningful Use, ICD-10, more and more top down "big data" standards and approaches, that focus on qualitative data entry AS care. I mean this literally: thanks Obama.
Doesn't basically everyone consider or day dream leaving their medium level job pretty often? What options are there people to make nurse level money in a regular town?
We've read similar reports about the "great resignation" with software engineers. Attrition is actually lower now than it was before the pandemic, so...
Cynicism and complaint is our zeitgeist. Answer me how many actually left in year prior if you want my attention.
Lots of considering leaving a profession, also considering losing fat on Jan 1, and saving for retirement.
When people are surveyed there is a big difference between why they say and why they actually are doing the action. For example "Yeah, covid has been tough... and those insurance companies though... And doctors really dont respect my profession... Oh my [pregnancy/parental leave/dream of being a DJ]? yeah that has nothing to do with it."
These kinds of opinion surveys are just barely "science" .
I work at a startup* trying to tackle nurse burnout, and two of my family members are nurses. Here are a few things I've learned:
- Nurses were getting burned out before the pandemic, and the US has a nursing shortage that's been going on for about 90 years (it started with an infrastructure buildout in the 1930s).* So it's a secular problem, with chronic as well as acute causal factors.
- There is a ladder of nursing credentials, and the shortage effects them differently. Hiring for roles like CNA and LPN/LVN has exploded because of the shortage of RNs and above. CNAs get trained in 4-12 weeks to do the heavy lifting of care; RNs get ~3 year degrees to perform much more complicated tasks.
- Burnout, and the nursing shortage, are in a positive feedback loop/downward spiral. That is, the more nurses burn out, the more they cause other nurses to burn out. Short-staffed facilities have a very hard time pulling back to normal staffing, because nobody wants to join a skeleton crew. (I know of long-term care facilities where the scheduling nurses (the bosses) are working the graveyard shift because they can't fill it.)
- Many nurses work rigid schedules on 12-14 shifts, and a lot of medical errors happen at the end of those shifts. **
- The hot US job market (Great resignation, great reshuffle) is hitting nursing especially hard; it is very sensitive to external shocks. There are paths to easier work and higher pay.
- Many healthcare facilities and systems don't give nurses flexibility or the possibility of advancement. (One family member will need to quit her current job and come back in a year or two to her current employer if she wants to move up a pay grade -- which is like some tech companies -- but slower moving and lower paying.)
- Many facilities are run entirely on foreign staff (the H2-B visa allows that). And many nurses are imported from the Philippines.
Find it a bit amazing that so many here act as if the past two years are the sole reason.
Few people have been as relentlessly toxic and unforgiving on social media as nurses.
As a child of a nurse, that job has sucked for at least the past 40 years.
The pay is average.
Workplace is a cesspool of gossip and toxic work culture.
Management is generally terrible.
Also, the pandemic has exposed how many in the profession really are just narcissists.
The amount of facebook posts from indignant nurses spreading the most horrible comments , just to receive likes and be perceived as heroes, these past two years have made my stomach turn.
Its about time we cleaned up in healthcare.
Not just aduquate pay, making sure we properly manage healthcare professionals and evolve healthcare management to grow where its needed.
I am 100% positive a flexible healthcare system that expands and shrinks after societal need is possible.
Not this crazy old fashioned fixed set of beds for x or y, that gets cut in some wave when they are needed less. Only to cause havoc in years when they are needed more.
Make sure the good nurses dont burn out and quit leaving the narcissist and ego maniacs behind.
There are amazing nurses out there, but we need to face that many of them are absolute shit at their jobs. And should seek other venues.
This exodus may be a good thing in the end.
Hrmmm. Pretty sure if 90% of nurses actually left the profession it would be a serious problem.
That being said, I would be surprised if this actually happened. If even 5% left the profession would probably become more lucrative, since pay would have to rise to retain those who remain. Meanwhile, although nursing is not super highly compensated, the alternatives for someone who has only a nursing education and skillset will likely be worse. That may lead to a gap in ideation about leaving vs actually leaving, because the fact of the matter is that we all still have to put food on the table.
Funny enough, not a nurse, but took over a 2 year "sabbatical" to do COVID testing and Vaccination. As someone who is used to making design decisions on an EHR in previous consulting engagements, it was beyond enlightening to see how things are where the rubber meets the road. Was only a Clinical Health Tech and a Medical Assistant, but frankly burned out enough to move back to software work.
Saddest thing is that I really felt I was helping, but have to admit I've become burnt out in the healthcare field - Just have $500 or so in scrubs invested...
Taking the time has hurt my career in many ways, I do believe. I have a ton of respect for many nurses, but many travelers are worse than you might imagine. Over-extended, far over-paid for their work. And really don't care about the facility they are working with (or throwing others under the bus to cover up their own mistakes)...
It was a valuable thing to experience, and I do believe I helped many people, but it's a very different thing to be at the bottom rung than the one designing and implementing various systems. God forbid someone can see a workflow issue, propose multiple solutions, and have travelers ignore it because the workflow issue makes them more money.
Not a rant against nurses at all - As someone with over 20 years in various roles of engineering, it was quite an eye opener to me.
I see a lot of people mentioning the poor working conditions of healthcare professionals. Things like low pay, long hours, mean patients, etc. These are undoubtedly all problems that largely fall on the shoulders of nurses.
The issue with entitled, mean patients strikes me. While I'm sure a fair bit of this is due to the way in which misinformation about COVID and other health issues spreads on social media, I have a hard time believing this is the primary cause of this grumpiness. It seems more likely that the average person is just fed up being taken to town by a completely inhumane system that really ought to be the most humane of systems. Nurses are the front line representatives of a system that exploits people when they are most vulnerable.
Now, I'm not saying nurses deserve this at all. They're not to blame for the state of things. But the observation might go some ways in explaining the psychology of the phenomenon.
Being a physician, Since IT came, it has alleviated some problems but has unleashed a monster which tend to cause lot more data driven to documentation to burnout. Every physician in United States currently experiences some kind of burn out. Nurses on the other hand experience much worse, 12-14 hrs shifts of constant stress. Overall health system in US is broken just as the insurance system. People will leave jobs when there is no satisfaction and just burn out.
In my opinion nurse should have shorter 8 hrs shifts and 4 per week . In this capitalistic driven health care system, where being a patient and health care provider comes with a cost.
It cost something like 15% of the nursing workforce, people who were already Covid immune, since they had worked the Covid front lines from day one.
But we pretended the vaccine helped stop the spread of Covid. It doesn't. And we pretended the vaccine had no meaningful risks. It does. And we pretended that natural (recovery) immunity didn't exist. It not only exists, but it's far stronger than anything a vaccine can do.
And yet we pretended anyway. And now we're paying the price. Pretending makes for bad public policy.
There are a lot of things we need to stop pretending about.
My wife was/is both an RN and a DNP in NYC during the entirety of the pandemic. I'm an Iraq infantry veteran. Our experiences are remarkably similar and there are major trends as to why there is unsustainable turnover.
1. Everyone pays lip service. People stand at airports and say thank you for your service the same way they open their windows at 7PM and start clapping and cheering during shift turnover. Sometimes they'll say they know people who are veterans or 'frontline healthcare workers' as a sign of solidarity
2. Nobody actually wants to hear what you went through. Hearing people die or knowing people are about to die in sometimes painful, unfortunate ways is too raw for people to try to seek out and understand, despite the fact that for a significant portion of the population that's how we're going to go out, in a hospital with all sorts of drugs pumped into our system
3. There's a constant barrage of emotional/mental harm. Believe it or not, you don't magically 'harden up' immediately. Absorbing/witnessing drastic outcomes gets easier, but the burden doesn't get lighter. This isn't to mention physical harm. People do all sorts of things out of desperation and frustration.
4. The systems that manage you are byzantine if not kafkaesque. You're never sure how the decisions are made, yet you're the one that will be paying the most for it. You know deep down that you're just a number on a spreadsheet, and the only reason that keeps you going is internal motivation to do what you think is right, so you push on
5. The people who can help rarely think about you. Very few politicians will mention your name or your union that is doing its best to get some kind of safe nurse:patient ratios or even get the hospital to pay for your scrubs that they mandate. Very few billionaires have mentioned healthcare workers or veterans at all. As a whole, until someone has an emergency that threatens their physical or financial status, healthcare and security is treated as a black box with unreal expectations and extra sensitivity to deviations from said expectations, despite a complete lack of introspection and information on how those expectations came to be
I don't know what the solution is. In healthcare, every system is so deeply connected to the rest that destroying one or even refactoring takes down everything else, and we need it to stay online. The same applies to the continuation of geopolitics by other means. You can give every IC the best EMR system, the best rifle and radio, the best monitor/laptop/keyboard, but it's all for nothing if the system as a whole is a dumpster fire. Her frustration is palpable every time she finishes a rough shift (probably 2 out of 3), and the best I can do is lend my ear and pour a glass of wine.
That being said, I am grateful that she is continuing on the path. Our shared experiences have brought us closer than ever.
My wife is an ICU physician, so I've been watching this from the sidelines. I can't emphasize enough on how badly COVID broke the system. There's always been problem with staffing and burnout. However, COVID really brought out the worst in people. The patient population became far more abusive than it had in the past and this was during a period where all healthcare providers were working extremely hard, not seeing their families, and sacrificing their personal health to help people. Then, a large part of society decided that COVID wasn't an issue, refused to mask, and refused to vaccinate. At some point, a large portion of providers decided enough was enough and quit:
Now, the problem is that when people started quitting, there were fewer nurses to take care of the patients and their ratios went up. During normal times, a floor nurse might be 6-8 patients to one nurse, a step down unit might be 4-1, and an ICU might be 1-1 or 1-2. It depends on the level of care required. Now, they're doing more than double this on a regular basis. And, frankly, they can't do it, at least safely. There's a number that a nurse can call if they believe they have an unsafe number of patients in order to get some kind of legal protection, but they still have to see that number of patients. And, frankly, it's incredibly stressful because they really, truly can't take care of that many patients, so they quit. A friend of my wife is a nurse trainer at a large hospital. They're having 80% of new nurses quit during their onboarding process because the ratios are absurd. A good portion of my wife's time is spent figuring out who's the least sick patient to discharge from the ICU because they don't have the staff.
Unfortunately, I don't think we're even close for this to being over either. The constant refrain is that COVID is the new normal and we need to adjust. I would contend that a new normal would imply a stable operating point and I do not believe this to be the case. It's going to take a really long time to restaff appropriately where the patient ratios and stress level manageable. Long time means years because, really, hospitals want and need BSNs and not just associates level training. In the mean time, every time we have a COVID surge, the hospital gets flooded, everyone gets overworked and abused, and more people quit.
This is a topic that I'm pretty close to. After programming for four years in the Bay Area, I decided to become a nurse. I spent three and a half years bedside nursing before returning to coding: two and a half at the Cleveland Clinic (a respected hospital) and another year doing 13-week travel contracts across the US. My goal was to find problems affecting nurses that might be solvable through programming. After my time on the floor, I've come to see that the deeper issues are more structural and organizational in nature.
One fundamental force in nursing is that a nursing shift is unpredictable. Some shifts go very smoothly, some are absolute trainwrecks. Patients are, definitionally, sick enough to be in a hospital, and they can start declining very quickly. This means that whatever you are doing at any given moment is often interrupted by a new priority that must be handled RIGHT NOW. It means that your 'plan of attack' for the day (which patients get [meds | baths | food | mobility | turns | dressing changes] when) is often delayed, sometimes by several hours. Any number of things could push the schedule back - incontinence care, a doctor stopping by to discuss a patient with you, a patient fall, a medical emergency, a lonely patient. A few curveballs can put you way into the weeds.
Consequently, the culture on a floor is key to how good your shift is gonna be. If you help others out when you have some slack and they help you out in turn when you are behind, it really smooths out those rough days. If other nurses let you drown, you drown.
The biggest thing that a hospital can do to help nurses is to adequately staff their floors. If everyone is drowning because the floor is understaffed, no one has time to help each other. If you're caring for six patients instead of four (on a med-surge floor), there are days where there literally isn't enough time to do all the nursing care everyone deserves. Documentation can be, and often is, done after passing off your patients in report. After you've already "dropped" documentation from your during-shift schedule, patient mobility - getting people up and walking, or even just sitting up in a chair for meals - is the usually the next thing go. After that, hygiene. Nobody dies if they don't get a bath, but another patient certainly could die if you don't do X. Next up comes pain medication requests and incontinence care. For me, it was enormously stressful not being able to provide the quality of care that the patients deserve.
This can be a huge factor in burnout. The pandemic made things worse in a bunch of different ways. Besides the stress of caring for patients with a deadly virus, you also now have to add on several minutes to every patient interaction for donning and doffing PPE. That's even less time to do the nursing part of the job while you're dealing with a more critical patient population (who will need more care). Burnout rates increase and nurses leave, either leaving the profession or taking contracts that, even if the conditions are no better or much worse), at least pay a premium. Hospitals that were well-staffed face staffing shortages, and hospitals that were already short on staff are now in a staffing crisis. The hospitals have to spring for travel contracts, and the nurses that did stay are angrier that other nurses are making multiples of their pay for doing the same work.
Given that this thread has some 900+ comments already, this comment will start off pretty far down the list. But I see some people mentioning that you are working on trying to make things better for nurses - I'm guessing that those people will read the thread more thoroughly. I would love to chat with you about whatever it is that your startup / company / weekend hackathon project is doing in this space. I've dedicated five years of my life to the problem space and would happily share my thoughts and experiences.
Efficient systems are brittle systems. You wring all the slack out of it and any shock is going to cause failure. In this case, the slack is the nurses and other healthcare workers' mental health and burnout limits and pay and culture etc. etc. The slack is being pulled to lower costs and increase insurance/hospital profits.
It's unsurprising that what has happened in the past couple of years is putting stress on a system with the slack pulled out of it.
You're spot on. This pattern is emerging across many structures. Efficiency is inverse correlated with resiliency. JIT systems have spread over the globe but they don't handle shocks in the pipeline very well.
Cost optimization usually have huge gaps in things that are hard to measure like onboarding cost/time or morale or benefits of experience. Who cares about any of that when you can make the shareholders another million a the expense of literally everyone else?
If you have the opportunity to take a look at the content of your typical business administration book, or even the Harvard Business Review magazine, they essentially are collections of success stories. Instead of setting the narrative, they go and say “this or that worked/didn’t work, to get this company out of a slump”.
The issue, I believe, stems from the fact that “bringing in the MBAs” happens when a company doesn’t hit inflated targets, and for that you have to thank the c-suite, which isn’t necessarily a bunch of kids with master degrees.
In that content is the sometimes implicit, sometimes not-so-implicit understanding that efficiency is something positive. The very first thing a finance textbook will inform you of is that the market is efficient and that this is what allows it to function.
When in reality, efficiency and fragility are two sides of the same coin. You might not want to maximize your efficiency if you also want to be resilient.
I mean it's a capitalism problem. Get rid of MBAs, people are still going to want to maximize profits and eventually will start cutting personnel to do that. The entire system encourages that exactly, isn't profit the only reason anyone does any work?
Doesn't that pretty much start with the fact that Medicare pays far under cost? "Just stop optimizing costs" is a hard sell when a huge chunk of services are sold at a loss. Either optimize the business or go bankrupt.
think about this statement, good nurses are taking care of the people you love the most in their most helpless hours. how fucking cruel are we as a society for taking this type of love for granted? its just wrong to use people like that. nurses biggest psychological problem is that they ignore themselves and love others and take care of them better. i think its really shitty. like veterans of defensive wars.
The number of people in the US who continue to defend the abhorrent health insurance system is absolutely mind-boggling. The level of brainwashing that pervades discourse about single-payer health insurance being some sort of communist plot is testament to some of th emost successful propaganda of all time.
What's worse is it belies an ugly aspect of human nature (particularly pervasive in the US IME) that people absolutely do not give a fuck about anyone else when it comes down to it. As long as someone is fortunate enough to have decent health insurance through their job, people who don't are lazy.
The big picture here is that the wealthy want people dependent on jobs and to be in debt (eg student debt) because it makes them compliant.
So I'm not surprised nurses are leaving. Insurance companies make providing healthcare an absolutely miserable business and deliberately killing people ("prior authorizations", "pre-existing conditions", etc) should not be the basis for commercial enterprise. Denying someone life-saving or life-changing care should not be a profit motive.
What's worse is that a lot of the burnout is effectively caused by people who are profoundly selfish and are voluntarily choosing to get sick and die of what is now a highly preventible disease.
It's a hard situation because people depend on nurses so collectively they're torn. Teachers OTOH aren't life-critical (but still obviously important) so I'd actually like to see them make a mass exodus over all the right-wing censorship they're facing in most states.
Yeah it's wild how well the grift works. My coworkers want private insurance (because we get it) and oppose universal healthcare. I think generally people in the states are ok with a grift if it hurts poor people worse. Because of that literally everyone expects they are getting grifted at all times and trusts no one.
Most people work for money so I would take all this with a grain of salt. If you are a RN what are you going to do if not nursing? The same applies to all fields including Physicians.
Being able to do it doesn't mean someone will hire you. Almost anyone may be able to become an engineer but you hardly have a prayer of being hired for a well compensated and benefited role unless you have years of experience or a (science or engineering) degree combined with internship(s).
Both physicians and nurses have a lot of options beyond working at a hospital. Private practice, small clinics, education, consulting, etc. People who will be leaving in these next few years won't necessarily be retiring.
There’s a huge labor shortage, they could do just about anything and get a pretty sizable bonus to sign up. I’ve heard $20k bonus for trucking, local transit agency is offering 7.5k to sign up as a bus driver, police nationwide are desperate and the requirements for the local agency consist of any 2 year degree + being willing to be drug tested, construction industry is trying to recruit women now, etc.
Probably true in certain areas, but nurses are unique in that they occupy one of the few high-wage jobs in rural areas. Nurses, on average, are probably more likely to be in places where it is difficult to find alternative jobs of equal pay.
If you're a typical white-collar professional in say some business/science/engineering field you'll typically, unlike nurses, live somewhere with abundant other high wage jobs.
I’m not a nurse, so grain of salt and all that, but I think I’d rather be a nurse than any of those things. And except for (some) trucking, RNs generally get paid more than all of them, I think.
There’s a lot of white collar work that only requires a nonspecific college degree, but I’m not aware of such a high demand for for HR staff or accounts payable specialists.
One interesting thing to spot-check in this study would be geographic distribution.
Salary for nurses varies widely, and in some places, they're wage-competitive with Amazon delivery drivers now. I can easily see people deciding that even though they like helping folks, getting paid less than the people who drive around and drop packages all day doesn't seem like a fair deal.
Whether or not any particular nurse follows through with thoughts of quitting, all else being equal I think we want nurses who enjoy and want to stay being nurses rather than nurses who are thinking about quitting. Nurses who are happy provide better care than nurses who are so unhappy they want to quit.
Typically nurses are women. Typically women are married to men. Men worthy of a relationship or marriage to begin with typically have an income significantly higher than min wage, potentially capable of sustaining a family on his own. Nurses are women usually and women have options, usually.
This comment is kooky. Are you implying that one option for women nurses is marrying a higher-income man and becoming a stay-at-home spouse?
Men making less than the median for their gender (something like $55k in the US) are still marriageable; plenty of women marry men who can’t support families on their salary alone. Even at the median salary, supporting two people — let alone a larger family — could be a struggle, depending on debts and other commitments.
And then there are women who are not married to a man who makes money, either because they remain unmarried or because their husband has lost his job or cannot work for some reason.
Further, even if the cards align, it’s not great to be in a position of dependence on your spouse's salary. Sometimes you have to split up and sometimes your spouse dies without leaving significant insurance or inheritance.
I think they're saying that married people might have a little more leeway in changing careers because they have the stability of a second income in their household already.
It sounds like they're just being overworked. So, just have the nurses take a 20 minute break every 2 hours, to go out and take a walk. The hospital can require it if it comes to that but why wouldn't they just want to do it? and if the hospital doesn't want to do it, then the nurses should insist on it and walk off the job if not given their breaks. I would imagine the hospital would rather agree to 20 min breaks every 2 hours rather than loosing 90% of their workforce forever: they don't have a choice, they have to agree.
why doesn't collective bargaining work in this scenario? if the demand for nurse labor is so incredibly high, they should have a lot more bargaining power, no?
In my experience, most nurses come in, socialise and cheer you up, take your blood pressure and temperature with automated devices, that one can buy for home use, and give you medicines that a doctor has prescribed (someone can also can do at home if they are feeling up to it). This is a wonderful profession and they should be highly paid but do they really need a bachelor's degree or master's degree to do this job? Some specialised nurses can even draw blood but, again in my experience, many of those were unable to "find a vein" and had to call on someone more experienced or a doctor. Pretty sure some experienced heroin users could do a better job at this. Just my experience.
Where a less credentialed person can do the job it has already been done. Here's how it breaks down:
Registered Nurse (RN): The 'specialized nurses' you talk of, and what this article is mainly about. Requires at least an associate's degree to be licensed, but increasingly an bachelor's is expected. Only they can administer any medication a doctor prescribes, and only they can assess your condition.
Licensed Practical Nurse (LPN): If they are certified they can also do blood draws. Requires graduation from an LPN program (usually about one year) to be licensed. They perform easily predicted tasks like a dressing change that do not require assessment. They can also administer some drugs based on the situation.
Unlicensed Assistive Personnel (UAP): In a big hospital, these are who are checking your temperature most of the time. They can only do basic tasks that do not require any medical training, even if their experience is larger than the RNs and LPNs they're under.
There are also many different technicians. In a big hospital, an RN acts as a middle manager delegating their work to these many different tiers. In an ICU, or in a small hospital, it will be done much more by themselves.
Nurses complain about their work conditions, but I don't understand them. They had this massive leverage during the pandemic to discuss improvements. Some people may say "Oh but it is illegal for nurses to strike in country X", but what will governments and companies realistically do if all nurses decide to stop, arrest everyone and let the health system collapse? Not a reasonable option.
There's just something masochist about their profession.
It seems like your comment would be better directed towards weak or absent nurse unions, instead of individuals. I had countless nurse and physician friends go to their hospital directors/HR/managers during the pandemic "I need a raise because I have absorbed the load of 3 other workers and am working harder than ever." Not only were they refused, many instead received 10-33% pay cuts, with hospitals citing increased Opex costs despite decreased staffing, significant government assistance, and increased volunteer (0-cost) help.
It'd also be enlightening for people in this thread to have hospital executives explain how they have some of the highest patient numbers in history yet they're hemorrhaging so much money their physicians had to take pay cuts.
Nurses, due to their profession having relatively low barriers to entry yet requiring years of operational knowledge to truly be effective, need collective bargaining. Nurses do strike, and nurse strikes are actively occurring on the U.S. West Coast. However, the unions they represent are small and have little power overall. For a strike to be successful you need solidarity from a majority of workers in the area you want to impact. You also need buy-in from the hospital/region that union nurses will provide superior care to non-union nurses. Something that's hard to do when your average executive thinks that the most complicated thing a nurse does is sticking a patient.
It's unfortunate to see this downvoted because I've heard this sentiment echo'ed a lot and I think it's worth explaining.
It's not about the illegality, it's really just about people dying. Yes you can go on a strike but your patient that's in critical condition won't survive on principle. You could say "just don't care about the patient and strike anyway", but that's extremely hard to do.
Striking when it hurts some millionaire owner is one thing, you wouldn't feel bad about yourself. Striking when it hurts someone post-op who did nothing wrong aside from being sick isn't noble, you get to live with the fact that as an individual you could have saved them, yet you didn't because you wanted money.
Legalities aside, how would you feel about refusing to work for poor pay/conditions if you knew for a fact that said decision would result in many deaths?
Not a chance, not a speculation, but absolute awareness of the number of patients that will not receive care and likewise will die as a result.
I don’t think it’s fair to blame nurses for poor treatment when they have a multitude of terrible options to pursue in order to improve their working conditions.
I know Ontario all too well. The same people that depend on nurses won't do more than needlessly beat pots and pans for their "heros". They do not even support them with their votes, which put in power the nefarious Conservative party.
Who exactly are the nurses standing for? People that won't have their back.
{kind=link}
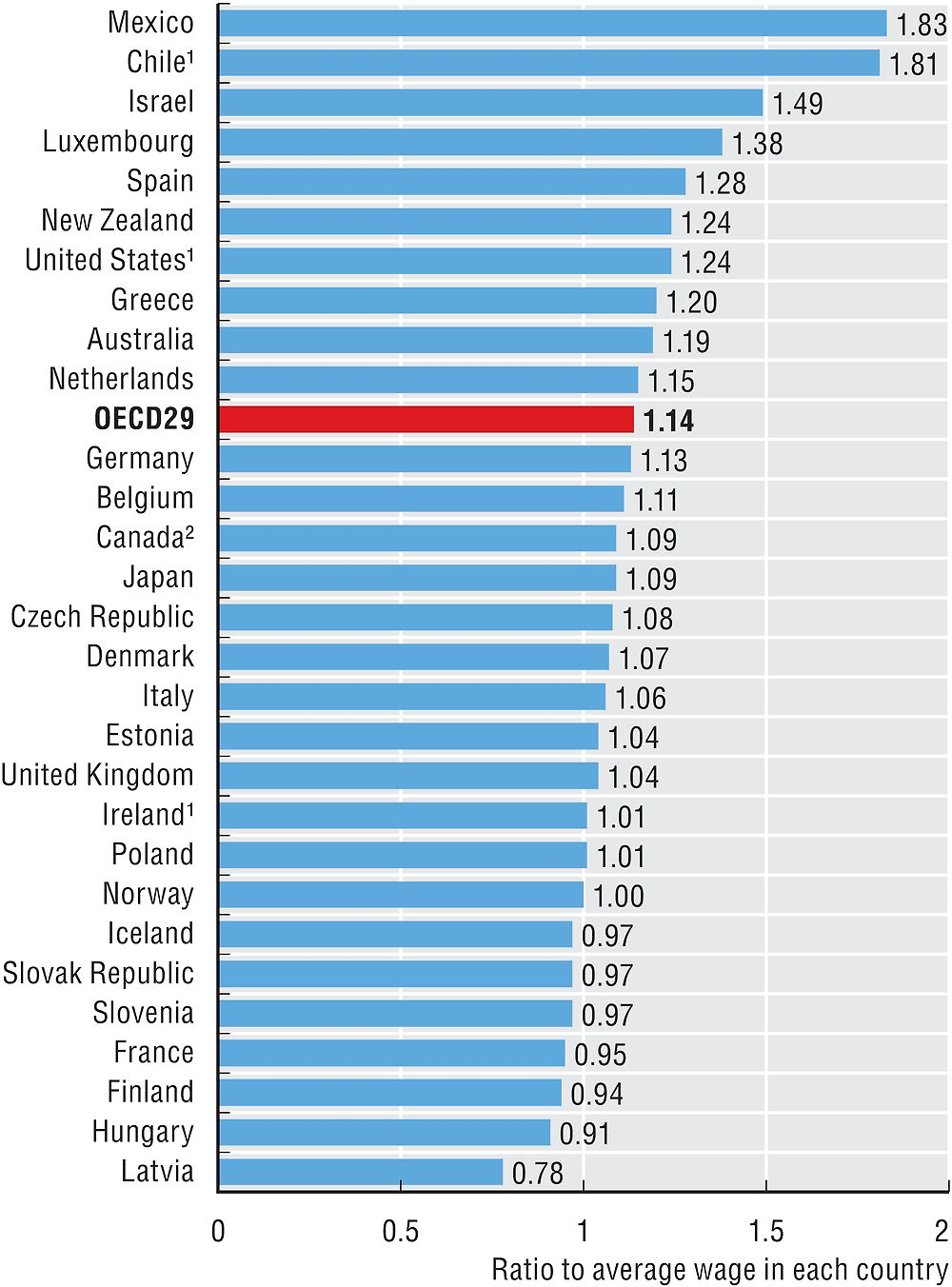{kind=link}
{kind=link}
{kind=link}
1. Many new nurses make the same or more and long time nurses. It's frustrating when the nurse in charge with the most experience is making less than new nurses. Some hospitals are even trying to stop nurses from talking about pay.
2. Patients in COVID have become downright mean. Add this to the problems nurses have management and doctors (who are often rude and arrogant) and it's a poor culture. The quality of the environment, from a mental health standpoint, is on the decline.
3. IT systems that they have to use were designed by people who have not talked with the workers who use them. They may have been designed with laws and compliance in mind. Nurses aren't the people who choose or pay for these systems. But, they use them a lot (maybe the most) and it's obvious they weren't taken into account when designing the UX. It's maddening for them.
This one is big for product designers. Often we listen to the people who pay for it and miss out on the people who actually have to use it.
4. Nurses are the catch all for jobs. Not enough aides? Nurses do the work. Food service workers don't want to take food into a patients room... nurses will do it. Not only do they have higher ratios of patients but they fill in the work when other areas have shortages, too. So, the work per patient goes up. Pay doesn't go up, though.