To be fair, Johnson & Johnson (a US company) also made a similar pledge to AstraZeneca.
These two companies have collectively received more than $1.5 billion from the US government [1]. As I understand it, Pfizer have not taken any federal funding. They do have government purchase agreements, but they are dependent on Pfizer delivering a viable vaccine. Their partner BioNTech received German government funding:
Berlin gave the German company $445 million in an agreement in September to help accelerate the vaccine by building out manufacturing and development capacity in its home market. [2]
I don’t think the data bears this out exactly. US healthcare tends to optimize for access and quality to the detriment to cost. As the saying goes: access, quality, or cost... you only get to choose two.
The US tends to measure better than any comparable country of its size on those two metrics (and quite poorly on cost...but some of that is because the US funds about 50% of worldwide medical R&D)
The US healthcare is good only when considering those who can pay to access it. But since large swathes of the US population cannot afford to have access (expensive insurance costs, even with Obamacare support), this becomes a mute point. If that is the metric, then even Brazil (and many other 3rd word countries) also has good medical care, because it works for the small percent of the population with money to access it.
And in fact this is one of the big differentiators between 1st world and 3rd world countries: if the population has access to quality services, in health care or other important areas like education and sanitation. The US seems to be designing its systems to become a big 3rd world country.
> The US healthcare is good only when considering those who can pay to access it.
False: The third leading cause of death in the US is believed to be preventable medical errors. You can go to the best institutions in the US to get care, along with seeing the very best doctors, but you cannot evade a statistic like that, even if you are in the 1%. See: https://www.npr.org/sections/health-shots/2016/05/03/4766361...
The truth is that you can be in the top 1%, sitting on a mountain of cash, and still lose an unfathomable amount of money, even while insured, if you have cancer or a rare disease. Both of which are actually common.
It is not the doctors who are the problem here with respect to the medical errors: it’s the healthcare system. A good read on what’s wrong with the system is the short book Our Malady by Timothy Snyder.
If you want to stay alive long term, you may want to consult HealthData.org which analyzes each country’s healthcare systems in depth along with outcomes. The group is world renowned. Ironically, it is also the IMHE group that does the coronavirus statistics that everyone consults.
Personally, I am an American culturally, but I became an EU citizen (Croatia) over the US healthcare system. I never plan on working in the US. I do select the country I am working in now due to healthcare.
Your points are baked into the data that I linked. The metric within is "HAQ Index" which stands for "Healthcare Access and Quality". I.e., access is part of the measure. In the US everybody has access, which is part of the problem that drives costs higher.
E.g., if you don't have insurance you can walk into an emergency room and get treated even if it's not an emergent situation. If you don't have insurance, there is a higher risk you won't pay. That cost then gets spread to others who do.
You probably don't know how the US system works. The only access that is guaranteed by law is to emergency services. If you don't have a paid insurance (through your employer or yourself), then you cannot access preventive care or otherwise normal medical consultation. Millions of people in the US don't have access.
For example, if someone needs to treat cancer, it doesn't make any good to go to an emergency unit: they will discharge the patient as it is not an emergency situation.
>if someone needs to treat cancer, it doesn't make any good to go to an emergency unit
That's because the ER is meant to stabilize a patient, not cure chronic disease. Which is to my point: people will forgo preventative medicine until their condition deteriorates and they need to be stabilized in an ER. People get their non-emergent conditions treated all the time in American emergency rooms.
E.g., if I have diabetes, an ER will not put me on a long-term treatment plan. But if I ignore my disease until I start having hypoglycemic symptoms an ER will treat me until I am stabilized enough to be released. Is this the best system? Absolutely not, but it's much different than saying "only the rich have access to healthcare".
FWIW, I used to work in healthcare, including redesigning ER processes
And how would anyone know if he has diabetes (for example) if the person doesn't have regular visits to medical facilities? In such a case they will go to emergency only when an emergency happens, probably when it is already too late. By saying that such a person has access to health care, you're just redefining health care to "emergency health care".
If this was not enough, hospitals are catching up to the "loopholes" in the law and abandoning poor neighborhoods, to make it even harder for people to use emergency rooms.
In the example of diabetes, many people are diagnosed when they show later term symptoms that require an ER visit. Since it's chronic, they won't be "cured" of the disease, meaning an ER can be their main mode of healthcare and the main mode of being diagnosed.
You may not understand the nuances of the article you referenced. Take Detroit, one of the cities used to support the claim in the article. The baseline decade used is the 1960s. Detroit has only about a third of the population it had in the 1960s so it's not rational to think they would maintain their previous healthcare infrastructure. Further, much of that population left for the suburbs of metro Detroit, meaning the healthcare facilities being built are just following the population demographics. Add onto that the point that healthcare has changed dramatically over the last 60 years with much more emphasis on outpatient care, and there are rational, non malevolent reasons to decrease the number of urban hospitals
Curious, in your healthcare experience, what would you estimate is the percentage of people who do have good insurance, but don't get preventative care by choice?
E.g. for myself, I have good insurance, but I don't have a "primary care doctor." I don't go to the doctor unless I'm injured or sick. And I don't mean a sniffle or cough, I mean sick as in I have felt awful for several days.
I don't think I have a good representative sample because facilities I worked for were a specific sub-population that would probably have a very high percentage that fall into the category of "no need for healthcare until something is broken or bleeding profusely"
With that said, it seems to be quite a bit and skewing higher for males than females.
If you have insurance and are not going for a routine exam once a year, you're doing a disservice to yourself because you miss the opportunity to catch issues that can be easily fixed when caught early but catastrophic if not. In fact many corporate policies require people to have regular exams exactly for this reason.
A lot of countries do not do “yearly physicals” like the American healthcare system recommends. This is because in countries with universal healthcare, patients within the country go to their GP/Primary Care Doctor far many more times on average than the typical American. So, in many countries, this practice is non-existent, basically because people just go to the doctor whenever they feel it is necessary—and far more often than the typical American does.
The average American sees a doctor 3 times per year. In France it is 6-7 times per year. In Japan, it’s 13 times per year. This statistic is directly linked to the cost of care.
In Europe, Canada, Australia, etc everyone has access. Why doesn’t access drive up their cost? Clearly access isn’t what is driving up the costs in the USA.
Because it's not as simple a model as "access vs. cost". It's access vs. quality vs. cost.
Canada's HAQ index in 2015 was 87.6 vs. 81.3 for the US. However, Canada spent about $27B US on R&D vs. $495B for the US. On a per capita basis, the US outspends most the world on medical R&D. That drives the US total healthcare costs up while helping to drive down the healthcare quality costs elsewhere. To a certain extent, the US subsidizes the healthcare costs through much of the world, effectively allowing them to optimize for a 2 parameter model while the U.S. must still deal with a 3 parameter model.
Yes, the US spends much more per-capita on medical R&D than other countries. But how do we know all this money is going into real R&D? How do we know most of it is not going into e.g. me-too drugs?
That's a potential real problem, but the concern should be across the board (i.e., how do we know other countries aren't funding me-too drugs) so it doesn't really help illuminate any disparity between countries (which is the context of this discussion).
I'm not trying to be dismissive, I just don't know how it's germane to the discussion unless we view all the other data through the same lens. The data I linked is per country in absolute and per capita basis that tries to put it in unbiased terms.
Are you claiming the US is disproportionately funding non-useful research? If so, how do we measure "useful" research funding?
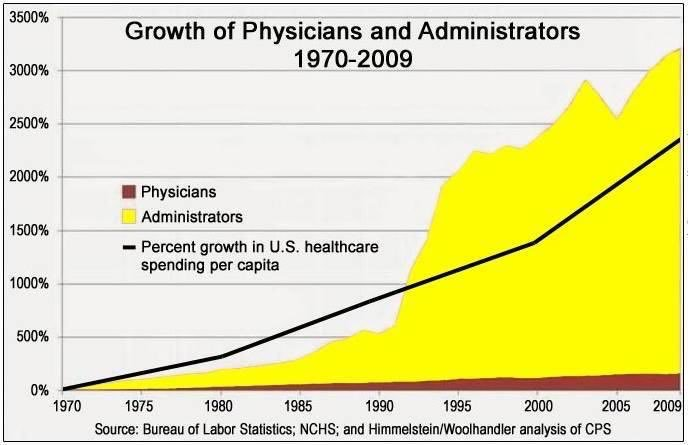
I do not know how to objectively measure useful research funding. However, this discussion reminded me of a graph I saw on the wtfhappenedin1971.com site [1]. It's not direct measurement of R&D development, but it sure as hell doesn't paint a good picture for all the spending that's going on. I wouldn't be surprised if a similar allocation of funds was happening in medical R&D as well.
Yes, I'm familiar with that graph. There's a similar one for college tuition in the U.S.; interesting that both are industries where costs have been growing at more than GDP year over year.
However, the point between comparing countries still holds. If you use older data, you'll see that the U.S. had even more disproportionate R&D funding
The important issue is that R&D spending is not a good measure of outcomes. A lot of R&D spending goes to high administrative salaries, equipment, facilities (real estate), and related costs that do not translate into outcomes.
What would you propose as a better metric of innovation?
I don't think there's a single perfect measure but if you put it in broader context of measures like Nobel prizes R&D spending, patents, etc. it does seem to paint the picture that the US disproportionately contributes to medical innovation.
It's very similar to the measure of health. There is no single great metric. Using a single metric like BMI or blood pressure is flawed. However, you can get a clearer picture if you bring together multiple metrics.
this is completely missing the point, people don't take chronic or slow-developing issues to the ER so they get worse and have catastrophic consequences resulting in both worse health outcomes and more expense because by the time they do come to ER it's a more serious intervention = $$$$
I addressed that in a different comment (I think we submitted comments at roughly the same time).
I completely agree that preventative healthcare is lacking, partly due to the system and partly due to culture. If the OP had originally said "preventative healthcare" I wouldn't have much to disagree on, but they used a blanket statement implying only the wealthy have access to healthcare in general.
The US also gives free preventative healthcare to many subsets of the population
As someone who migrated to Germany from Turkey, people like me (and everything we are involved in) are "German" when we do something they're[0] not proud of, we are "Turkish" if we ever come close to success, and "of Turkish descent" in the normal times. Of course it depends who you are asking :) It's a bit annoying to be honest but not a huge deal.
I didn't mean to make any judgment about the "Turkishness" or "Germanness" of Drs. Şahin and Türeci. I just mean to clarify that BioNTech was founded and is based in Germany, just as Google is an American company (not Russian-American) even though Sergey Brin was born in Moscow.
I have read it‘s a bigger problem and a source for islamism, especially for the 2nd or 3rd generation of descendents of immigrants: When Germans still see you as Turkish, but Turks see you as German, it makes sense to a) be angry and b) search for some other identity.
> The AstraZeneca vaccine also has 90 percent efficacy when used twice
No it doesn't. Both dosings use two shots, and the "90%" number from the smaller dosing is from an unreliably small sample set of 33 infections -- it could easily be 70-80% by next month when more data comes in.
I don't think we know based on public information. Some media report "up to 90%" which suggests the upper bound of the confidence interval, rather than the centre. Could also be a very wide CI, that overlaps with the standard dosage.
That's a fairer statement than the original which seemed biased towards only reporting the lower end of the interval without acknowledging the upper bound.
At the moment possibly wider error bars don’t come from just “33 infections” but more from possibly smaller number of those who received the observed treatment.
The bars are to be calculated using conditional probabilities.
>These two companies have collectively received more than $1.5 billion from the US government [1]. As I understand it, Pfizer have not taken any federal funding. They do have government purchase agreements, but they
So where did Pfizer's capital come from to shoulder these costs? It didn't come out of thin air, they've accumulated capital from somewhere. If not from taxpayers, someone is subsidizing Pfizer's expenses through Pfizer's revenue stream. Taxpayer subsidies really make sense here seeing how this issue effects everyone.
> someone is subsidizing Pfizer's expenses through Pfizer's revenue stream
Companies taking a portion of what they earn from their existing products and investing this money to create new products is beneficial, and we should have more of it.
Additionally, while this is probably not the case for Pfizer, another possibility is that a company can take outside investment to fund development of a new product.
Not the OP, but what she/he is probably hinting at is that the majority of Western Governments (i.e. both the US and the EU) have poured trillions of dollars/euros into the market as the pandemic started, money that has helped the capital markets stay afloat (and even more than that).
Without those trillions of dollars/euros most probably the capital markets would have been down by at least 50% (my guesstimate, or at least that's where we were headed mid-March), which means that the money available to companies like Pfizer would have been a lot less.
As such, Pfizer saying that they didn't receive federal money is technically correct, but without federal money most probably their market value would have been a lot less right now.
A 40-50% reduction in share price would have most probably eliminated the dividends completely, especially in a very adverse deflationary market, which most definitely would have seen the most of that $10 billion sum allocated to other things than R&D.
Pfizer's cash situation or ability to spend/pay a dividend has nothing to do with stock price. Pfizer does not have their cash balance invested in other stocks. Ability/willingness to pay a dividend has to do with excess cash.
To the extent there's any relation, it's a high stock price that discourages paying a dividend. If the dividend yield will be basically nothing, why bother spending down precious cash that could be reinvested (because obviously the market values future cash flows a lot more than current ones).
Deflation might encourage a little bit of holding of corporate cash rather than spending it on R&D, sure. But even then I think you're overstating the case.
The question was simply to stimulate a more holistic view of the example at hand: that Pfizer did this on their own and essentially didn't need/get any financial help. Sure, Pfizer didn't receive direct subsidy in the short term related to COVID R&D and is taking on risk.
But let's look at this more holistically. Pfizer and pharma benefit a reasonable amount from public research. Pfizer has received their fair share of governmental funding in the form of products, services, and research:
https://www.usaspending.gov/search/85a918fa6adf5152dbac723d2...
They've also been subsidized by people with illness over the years that isn't related to COVID (directly or through their insurance provider pools). It's in other cases the previously sick that have padded Pfizer's profit margins enough to enable them to accumulate enough capital they could take on this sort of risky R&D. Theres also the costs of enabling laws and defending their IP rights from external pressures the US pushes.
It may not be direct subsidy but there are plenty of indirect subsidies that enabled Pfizer to do this. Let's stop pretending these businesses pull themselves up by their bootstraps to success and take on all the risk: they don't. They very often take low risk returns and transfer to high risk and use subsidized activity (e.g. federally funded research) to their advantage. Anything high risk like pharma is prone to failure and needs assistance.
Should we continue assistance? Absolutely, I think so, it's good for everyone. As one parent mentioned, it is good to see these businesses reinvest in further R&D that lead to new discoveries in therapy and treatment as opposed to simply hoarding capital.
Apparently the thought of the narratives that Pfizer didn't pull themselves up by their bootstraps financially makes some people cranky. Everyone needs assistance (especially in high risk arenas), let's not pretend that assistance doesn't exist simply because its indirect, time delayed, and being shifted around.
I agree with your overall point that it needs to be looked at holistically, but I don't think I agree with your stance on some of the subsidy arguments.
A subsidy is, by definition, a governmental funding mechanism. "People with illness" who used Pfizer products in the past aren't subsidizing the COVID vaccine anymore than I subsidize an automobile manufacturer making pickups when I buy my tiny hatchback. It's built into the business model and not really a "subsidy".
I agree with you in terms that we shouldn't view these companies as operating in a vacuum, I just don't think the idea of the markets being propped up is the most congruent way of framing the discussion. Pfizer benefited along with most other publicly traded companies, irrespective of their COVID vaccine.
{kind=link}
These two companies have collectively received more than $1.5 billion from the US government [1]. As I understand it, Pfizer have not taken any federal funding. They do have government purchase agreements, but they are dependent on Pfizer delivering a viable vaccine. Their partner BioNTech received German government funding:
Berlin gave the German company $445 million in an agreement in September to help accelerate the vaccine by building out manufacturing and development capacity in its home market. [2]
[1] https://www.nytimes.com/2020/05/21/health/coronavirus-vaccin...
[2] https://www.bloomberg.com/news/articles/2020-11-09/pfizer-va...