There are some questions I haven't been able to find good answers to in addition to the one posed in the article:
1. Is it possible to get COVID-19 twice?
2. If (1) is true, are the symptoms the same (if applicable)?
3. If (1) is true are you still contagious?
4. There's evidence that there are multiple strains, can you get both strains?
5. What's the likelihood that a mutation will occur once treatment is more widespread?
6. Does the heat make it significantly less likely for you to get COVID-19?
My impression so far is that we'll never get rid of this thing, and at best this will be something like the seasonal flu, where we'll just have to live with it and great shots yearly.
No, doesn't seem to be, but you might still have "viral shedding" for a bit even after you are "recovered". meaning you could still be contagious.
4. There's evidence that there are multiple strains, can you get both strains?
You shouldn't think about them as multiple strains, as of now it is 1 disease.
5. What's the likelihood that a mutation will occur once treatment is more widespread?
Mutations occur all the time, there are already 10's of known mutations of virus, it doesn't mean there are 10 separate diseases.
6. Does the heat make it significantly less likely for you to get COVID-19?
There's some evidence warm weather slows spread for viruses like this, but we can't assume that about this virus yet. A good counterpoint is Qatar adding 258 cases in one day, it's hot there.
I used to live in that part of the world. Air conditioning and active cooling is pervasive there. In a sense, people's exposure to the overwhelming heat of the day is perhaps much more limited than you might expect.
Africa generally being a poorer continent also means a lot less travel to spread the disease, especially international travel from Asia and Europe, and the potential for local outbreaks to pass unnoticed due to lack of medical care, especially if symptoms for most young people are benign, and elderly people dying at the first sign of infection is a common occurrence
There could be less testing in Africa, so less confirmed cases. Here in New Zealand we have had only 5 cases with no increase in days, yet very close links to China and Australia and cool fall weather, making me wonder if and how many undiagnosed cases there are.
The case fatality rate is estimated at 2% - 3% but that is with medical care. Without ventilators and ICU care, CFR might rise to as high as 10%-15%. With its exponential growth rate, it'd be highly surprising for the virus to go unnoticed so long.
According to the Johns Hopkins doctor recently interviewed by Sam Harris (sorry, couldn’t find the name) the South Korean number is likely the more accurate one due to a higher prevalence of testing. The higher rates from other countries are essentially a denominator problem (I.e., with limited tests only the most sick are tested, leaving the only moderately sick untested and thus out of the calculation)
I've seen an infographic passed along, albeit on twitter, so authenticity is suspect --but it was comparing ages in SK and Italy of cases, where mortality is higher in Italy, because mean age was higher in Italy, a lot of the tests in SK were in churches where initial outbreaks were that were prevalently populated by youth...
2000x 20 year olds 2000x 60 year olds...and you're gonna have highly different results for CFR.
I'd say it's somewhere in the middle of both... maybe something like 1.5. But I'm not an epidemiologist, but if the age gaps matter then it could be about that... just my thoughts.
That's the estimated percentage of people who need some form of ICU treatment due to COVID-19. If there's no more ICU beds left, it's safe to assume that the majority of people in need of ICU treatment that can't get it will die.
You also have to add all the other patologies that will get affected by the lack of ICUs. All in all, 10% is a safe estimate. That's why flattening the curve is extremely important. The actual percentage in need of ICU will surely vary with time, but that's the important metric, because that's how many people will die when the health system saturates.
5% needing ITU was initial estimate. In Italy it’s 10% due to an elderly population. And some on ITU would survive without ITU but it does improve chances. You make good points, I’m mostly just saying there is a high degree of uncertainty
Multiple sources indicate that’s the severe percentage, and we know a bit about untreated ards.
Moreover, deaths from lack of capacity will not be limited to covid cases. And many of the current non-covid icu cases may be exposed to medical staff who are not being tested (in the USA) and die that way. This is what happens in nursing facilities like Seattle.
the ramp up isn't done, nor halfway yet, as italy hasn't reached inflection of the exponential curve yet. once the net new cases begins to steadily decrease the numbers are roughly half way to the final max.
But AC is very common in the US too. So shouldn't we expect spread in US summer to behave more like Qatar than Africa? Europe on the other hand may slow down since I think AC hasn't caught on to the same extent.
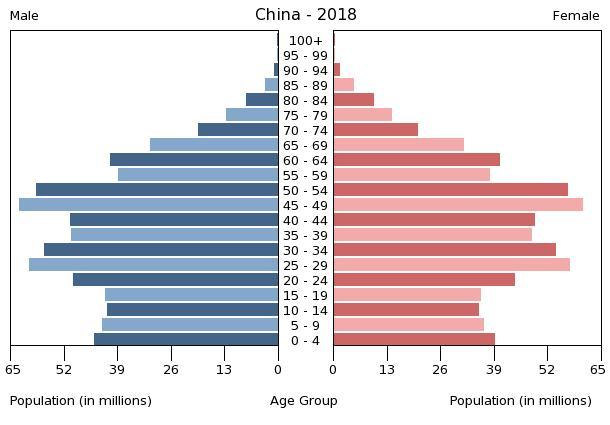
Demographics structure. E.g. in Nigeria 65+ old constitute ~3% of population, in Italy ~22%. Now compare that with COVID-19 severity and mortality age breakdown.
>> 5. What's the likelihood that a mutation will occur once treatment is more widespread?
> Mutations occur all the time, there are already 10's of known mutations of virus, it doesn't mean there are 10 separate diseases.
I agree, but I'd like to add more details. Most mutations are irrelevant, and if you have antibodies for the original version, the same antibody is useful for the new version.
From time to time, the mutation is in the part that encodes the part that is recognized by the antibody, and then you may be infected by the new version.
[There are a lot of other mutations. A lot of mutations just make the virus not able to reproduce, or break some important part, so the mutated version just disappear. Another mutations make the virus more effective or less effective, so they change how bad the symptoms are.]
Others may change how fatal the infection is (in either direction)
This is actually one of the reasons that viruses generally become less deadly the longer they circulate through a population. A less-deadly version will spread faster (by not killing it's hosts), and will tend to outcompete a deadlier version
We really should be increasing humidity in hospitals and offices in the winter. Newer planes have already been moving in that direction (to increase comfort).
> It is ABSOLUTE humidity which matters, not relative humidity.
This 2019 paper says that (i) in higher relative humidity, the fine droplets stay larger (larger size after evaporation down to the equilibrium size, given by Kelvin equation) and thus linger in the air for a shorter time. And (ii) higher temperatures, virus proteins denaturate a bit faster. The compound effect of higher relative humidity and higher temperature then makes it look like it correlates to higher absolute humidity.
Not sure how relevant it is, but influenza (flu) and common coronaviruses (common cold) are not in the same family. Anyways, it seems like it is not a good idea to speculate, even the viruses have closely related:
Also, spreading of flu during "flu season" is marked by holidays when long distance travel happens. This causes slightly different strains of the flu to be brought into regions where people do not have a natural defense to that strain.
Interesting tidbit I learned at a Town Meeting (streamed) yesterday. Winter Break in Massachusetts was instituted to halt the rapid spread of flu during the winter months. Kids would take it into school, spread it among themselves and bring it home to adults, who would get hit harder by it.
The winter break put an an incidental isolation in place that slowed the person-to-person spread down.
This is why schools have to close now to control the spread of COVID-19.
Hospitals worry about many microorganisms besides the coronavirus. It would be unwise to encourage the growth of bacteria and fungi to arrest one virus that can be controlled in other ways.
From my experience, I have always gotten the flu, or some kind of sickness, after the cold months, as it turns into spring and summer.
When a warmer spring month rolls around, I think that I must’ve escaped getting sick with the flu, then, bam!, I get hit with it, and get knocked out for a few days.
The annoying flu is during the summer, when it’s hot, and you’re sick, so you just become more miserable.
Abstract:
This paper investigates how air temperature and humidity influence the transmission of COVID-19. After estimating the serial interval of COVID-19 from 105 pairs of the virus carrier and the infected, we calculate the daily effective reproductive number, R, for each of all 100 Chinese cities with more than 40 cases. Using the daily R values from January 21 to 23, 2020 as proxies of non-intervened transmission intensity, we find, under a linear regression framework for 100 Chinese cities, high temperature and high relative humidity significantly reduce the transmission of COVID-19, respectively, even after controlling for population density and GDP per capita of cities. One degree Celsius increase in temperature and one percent increase in relative humidity lower R by 0.0383 and 0.0224, respectively. This result is consistent with the fact that the high temperature and high humidity significantly reduce the transmission of influenza. It indicates that the arrival of summer and rainy season in the northern hemisphere can effectively reduce the transmission of the COVID-19.
Doctors tend to be reluctant to extrapolate strong conclusions from relatively close R0 values like those presented because of the number of confounding factors. It’s really most valuable when looking at orders of magnitude difference (e.g., measles with an R0 of around 15 compared to seasonal flu with an R0 of around 1-3).
I didn’t see in that study much consideration of other variables and the p-value used for relative humidity was on the high side by publication standards (up to 10%)
Regarding Quatar (or any warm/hot place): Note that a significant fraction of people spends a lot of time inside. This means the temperature there is actually colder, there's less sunlight (especially UV), and people are closer to each other.
Also note that for the common cold, the reason that it spreads more during winter times is not primarily temperature, but the fact that people spend more time inside while ventilating (opening windows) less often.
Comparing speed of distribution in different countries is extremely difficult, as there are too many factors at play. The 258 cases in Qatar might have been 500 if it was colder there, no one can proof or refute that.
> The 258 cases in Qatar might have been 500 if it was colder there, no one can proof or refute that.
It certainly means hot weather won’t “stop” the virus, just slow it by (in your example) 50%. That’s not a lot of comfort, although it would buy some time.
I know that in places like Qatar and India, there is a tendency to use artificial cooling. (I'm pretty sure India is the single biggest growth market for air conditioning on the planet.) I'm just thinking, if a bunch of people gather in an air conditioned theater, would it even matter if it was 95 degrees outside? Just a thought.
I guess to really know, we'd have to wait and see what happens in places where it is hot, and humid, and artificial cooling is not so widespread? Like Sub-Saharan Africa.
> 6. Does the heat make it significantly less likely for you to get COVID-19?
There is actually another part of the world where it's summer. Australia's case count graph is displaying the standard hockey stick shape, so based on the typical growth rate we should know in a week or two.
Can you cite some sources for your responses to 1 and 4?
Re: 5, there's clearly a distinction between typical mutations, which have no particular effect on the virus' behavior but do allow us to trace infections, and behavioral mutations, which might allow reinfection or make the virus more or less contagious or deadly. I think GP is asking about the second kind, since they're also asking about reinfection. Maybe that's obvious, but considering that, are there sources saying that the evidence so far is that there is only one strain?
Re 6: this is an interesting question. My layman's understanding is that heat usually reduces the spread of disease in temperate climates both because the disease can't survive as well and because people spend more time outdoors and in less people-dense spaces. In somewhere really hot like Qatar, we would expect to see the opposite of the second effect; I'd think people would spend more time indoors with A/C when it's excessively hot outside, increasing transmission rates as the outside temperature rises.
This outbreak has made me realise how I've gone my whole adult life without knowing some basic things about bacteria and viruses. Like, I never knew about how soap dissolves the virus's outer coating...
Anyway apparently hot and wet is good for bacteria, but cold is better for viruses. The bit that made it click for me is that viruses aren't metabolising anything outside of the host-cell, so the best a virus can hope for is to not be destroyed -- and cold is a better preservative.
I'm still not sure whether hot and humid is better than hot and dry though? I think I read that hot and dry is worse, because it increases evaporation.
Qatar is more humid than people think for being a desert country, because it is a peninsula in the gulf. As I write this, it's about 70% relative humidity.
While there is evidence that viruses don't like heat, the main argument about wanting to flatten the peak until the warmer months is because the colder months also have correlation to other diseases.
This disease would spread the same in any weather but most countries would be able to cope better, hospitals have more space and people's immune systems would be stronger in the summer.
(Not a doctor.) In general it is possible to get the same infection twice, depending on circumstances like a weak immune system, not recovering properly after the first one etc. Whether this is true for ncov is most likely not scientifically proven yet, but even if, it is safe to assume that this happening is the exception.
All I've heard regarding #1 thus far is "we don't know". Do you have source that states otherwise? Based on the responses so far, I'm not alone in wanting to review it.
Mutating doesn't mean it's going to get worse. It's entirely possible for the virus to mutate into a less dangerous form. Going out of your way to get it now is too much of a risk.
While I don't believe SARS-CoV-2 is quite as bad as the media frenzy is making it out to be, it's absolutely a good idea to do everything you can to avoid getting it. The same goes for the flu and for colds. If you catch any of these, you may be OK, but you risk spreading it to people who won't be.
1-3% case fatality rate? 70% of the population expected to be infected.
That's ~1 out of every 100 people. This isn't just a media frenzy, by the end of this you WILL know someone who died as a result of (complications of) Coronavirus.
But its hard to believe they report infection rate properly. It may be 7% of those with symptoms (arriving at hospital)? Which is expected to be a 'cherry picked' subset and have a higher rate.
I think this is true for very lethal viruses that have risk of killing host before spreading.
For virus that can spread before any symptoms and long after symptoms disappear and survive so long on the objects and in the air I think there will be no evolutionary pressure to get milder.
And we can get harsher version just by random chance because this virus is so infectious that it has a lot of leniency whether and when to kill the host.
You will not find concrete answers online because this is a research area, scientists are not sure yet about how to answer these questions. And sometimes the existing answers are based on limited information or just misinformation.
If your immune system develops an antibody based on epitopes that differ in the second strain, I would think you could contract it again. Two people who overcome a virus may ultimately derive different antibodies, and some may do better at matching the class of viruses than others.
I don't think it's very common to be that unlucky in your own body's development of a suitable antibody.
At least, this is my understanding based on a recent microbiology course I took. Immune response is a fantastically complex thing.
Viral reinfection is a known thing. Immunology is just, well, really complicated. One person's antibodies may have worked against the same virus their family member's did, but not against some slightly mutated strain that arrives after circulating for a month. Or frankly, testing isn't perfect and it's possible he had the flu before and never had COVID-19 at all.
In general, populations as a whole develop herd immunity to viruses reasonably quickly. This process is understood. Individual case data is always crazy.
So: 1. Sometimes, 2. Probably, 3. Yes, 4. Maybe, 5. It'll definitely happen eventually, 6. Yes, almost certainly.
And indeed, it will never go away, just like H1N1 flus have continued to circulate ever since the 1918 pandemic. But after a while, immune response and vaccination regimes will turn it into a nuisance.
Its only been around a few months so hasn't had a chance to significantly mutate- and it hasn't needed to. As such its unlikely you'll get a second time any time soon, however in future years it could mutate.
There is very little known about this particular case - for instance what testing procedure were they using. It could be that the first test gave a false negative, or the second a false positive.
Dr. Vincent Racaniello, Ph.D. (@profvrr on twitter) is Higgins Professor of Microbiology & Immunology at Columbia University Medical Center. He has been studying viruses for over 40 years.
Dr Racaniello is also the host of the This Week in Virology podcast, which I highly recommend.
They've had a series of episodes on COVID-19 recently, all highly informative. Episode 590, the most recent one, debunked the "two strains" rumor that's been going around.
You can hear the episode here: [1] and read a transcript of the portion of the episode where the rumor was debunked here: [2]
I did some reading on coronaviruses and learned these viruses do not have reverse transcriptase, which would allow an RNA virus, like a coronavirus, to incorporate into the host genome, becoming a permanent resident. In other words, the viruses lack the machinery necessary to convert themselves into DNA and cannot cause a chronic infection.
That said, it is possible that people co-infected with another RNA virus expressing reverse transcriptase would allow the coronavirus to incorporate into the host genome
A plasmid does not 'integrate into the host genome'. The entire genome for human cells is stored inside the nucleus packaged as chromosomes. The plasmid exists outside of this, and just hijacks our replication machinery.
It's hard to appreciate without first understanding how our genetics work. That is, the mechanisms that are responsible for replicating our genomes and turning our genes into proteins.
Viruses are an inevitability because they exploit vulnerabilities in those mechanisms. Viruses are not alive. Instead a virus causes "live" modifications to a living organism which causes it to simply reproduce more of the virus. When you have a virus you are essentially one with the virus; a modified organism.
Retroviruses go one step further by permanently making that modification. Now you are forever modified with the extra functionality of producing more of that virus.
But the really beautiful thing is how minimal these viruses are. If you've played code golf you'll appreciate it. In the smaller RNA viruses like influenza and HIV, each virion carries around exactly what it needs to make those modifications and not much more. They consist of proteins which cause our cells to accept them as well as the genome which causes our cells to make more of those proteins. They also cause our cells to reproduce the genome itself too. Eventually the cells become full of virus stuff and somehow the viruses assemble themselves back into virion, the cell dies and releases the new virions.
The HIV genome is incredibly compact. It's the closest thing to design I've ever seen in biology. It packs more information into its genome than would normally be possible by utilising overlapping genes on the forward and reverse strand. It's quite remarkable just how clever, minimal and perfect it is.
These tests test for the presence of viral nucleic acid. You can still have detectable levels of viral nucleic acid in you after the infection has ended.
What actually matters is whether or not you have virus replicating in you. The presence of viral nucleic acid is an imperfect proxy for that.
I warned you a week ago we would "waste of resources" and here we are:
"Health officials are struggling with a complicated message — more people can get tested, but those with mild symptoms should stay home and practice social distancing. Some go so far as to warn that widespread testing at this point could threaten the U.S. response by burning through precious supplies just as a tidal wave of sick people descend on the system — a message at odds with administration announcements that millions of test kits are finally becoming available."
There are many cases of "false negative" with current testing kit.
Most probably, patient who almost recovered, received false negative result and has been released from quarantine still being contagious.
Partying with neighbors definitely was a bad idea.
We've asked you repeatedly to stop posting political (in this case nationalistic) flamebait to HN. If you keep doing it, we will have to ban you, so please stop.
And definitely please don't "make the same post again and again" about anything on HN. Repetition is the enemy of curiosity.
China's numbers don't pass any sort of "smell test." China is an absolutely massive country with a massive population. It's not possible to "totally lock down" a country this big and with so many towns and cities out in the boondocks. If you don't agree with me there I suggested you visit China and travel around and see the enormity of even their "provincial" cities.
How does it make any sense at all that in the place where this started, a place with 1.4B people, that over the last few days, only handfuls of people have tested positive? Fewer people than tested positive in Iceland? A country of 300k in the middle of the Atlantic...
One of my close friends is Chinese and her family live in the outskirts of Wuhan. I asked can her parents leave her house and so on and she told me they were never locked down so they couldn't leave home. So if people near Wuhan weren't "totally" locked down, how was the whole of China SO locked down that basically nobody got this virus in the past few days?
Does it make more sense that there was some sort of perfect miracle lockdown where all 1.4B people in China were "locked down" and didnt infect anyone, OR that China realizes that there is little attention on them right now and are playing down their numbers OR simply not testing people and letting everyone gawk at Italy and South Korea? China is using this as a propaganda exercise to demonstrate the superiority of their top down authoritarian way of government, so Western media is now praising a dictatorship which also happens to have concentration camps for muslims and silences political dissenters brutally.
The stories from expats in China line up pretty well with enforced social distancing across the whole country on a scale even South Korea hasn't tried yet. That doesn't mean the numbers will stay low forever (once the restrictions lift, you'd expect it to come back), but it is consistent with the numbers being low for now.
They aren't done with the virus, but the worst seems to be past. Whereas if it could easily re-infect then I would expect the case numbers to strictly increase.
I'm wondering if China is shooting itself in the foot by being on lockdown because they may just be delaying the inevitable now that it's pandemic and at risk of becoming endemic.
If we assume this will become endemic and a vaccine is a ways off, it would seem like the best approach is to flatten the curve just under the healthcare system capacity and get it to "pass through" most of society quickly (i.e. everyone who is at lower risk gets infected and quarantines until viral shedding stops).
Doing this would allow us to return the economy back to normal as quickly as possible and prevent all the fallout from an indefinitely stopped economy. Once most people have had it, we'll essentially end up in a state of herd immunity and it becomes statistically less likely than other health concerns at-risk populations had before COVID-19 was even a thing.
Meanwhile China, being on lockdown the entire time is still susceptible to having it become a pandemic within their own population as soon as they lift the lockdown and try to return to normal because they citizens haven't had the opportunity to develop antibodies as broadly.
Great find. Going to read up more on Patrick Vallance's plan.
This was an interesting point from a Guardian article where he defends the plan:
“If you suppress something very, very hard, when you release those measures it bounces back and it bounces back at the wrong time,” he said. The government is concerned that if not enough people catch the virus now, it will re-emerge in the winter, when the NHS is already overstretched. [0]
Thanks for posting this. I was initially very negative about the UK strategy yesterday, but on reflection today I think they may have a very sensible long term approach to the situation, although highly risky to balance correctly.
Even without it, we're doing a terrifying balancing act with the economy. We want a V-shaped recovery and the best way to achieve that is the swiftest resolution to pandemic.
A U-shaped recovery would be bad for a lot of people, especially if prolonged. Last thing we want is an L-shaped market with no real recovery.
But the healthcare system is overwhelmed almost immediately. Wouldn't it take both these hard measures and a lot of time just to get it in reach of healthcare capacity?
The condition can ONLY improve in terms of new cases, not deaths, 1) if there is a vaccine, 2) 40-50% people get infected and develop immunity, or 3) people start living in bubbles, including masks and gloves and stay away from each other, that there spread is controlled.
We know 1 and 2 have not happened. So either China is still in lockdown and this lockdown is how the life will be till there is a vaccine, or the data is not correct.
It could be that measures less severe than "masks and gloves and stay away from each other" are enough to bring R0 below 1. Maybe just not having people go out when sick with coronavirus is enough, and all the other measures are just a matter of bringing outbreaks to an end faster with a smaller peak. South Korea has definitively shown that the coronavirus can be controlled, even if you don't trust China.
> It could be that measures less severe than "masks and gloves and stay away from each other" are enough to bring R0 below 1.
That is a very good point. I think you're right, focusing on R0 is the right thing and that might just be the key since estimated R0 was ~1.x-3.x, so perhaps masks, gloves and some common sense can indeed bring it down to <1.
> With that even at 1% 6-8 million would have died.
That number assumes a homogeneous distribution. As deaths are observed mostly in the elderly and China's demographics tapers off rapidly beyond 60yo, the incidence would be far lower than 1% of the total population.
That assumes the death rate is actually 1%. In the hypothetical where 40%+ have been infected, I think it’s be safe to assume the death rate might be lower than we suspect it is.
It was the same during the H1N1 hysteria. CFRs being quoted of 2-3% and it turned out much less deadly than an average flu.
A few weeks ago we didn’t even know there were asymptomatic carriers. My prediction is that when all is said and done and the IFR is closer to 0.01% that this will all look very stupid.
Experts in Ohio say they suspect that 1% of people are infected. OK, so where are the hospital cases?
South Korea is doing some random testing to figure out how many cases only looking at symptomatic patients is missing. With that it looks like the total fatality ratio is just .6% for them. But of course they haven't had hospitals overwhelmed with too many patients at once and I expect that Italy will see a much higher fatality ratio.
At 0.01%, Italy would expect to see around 6,000 deaths. They're up to 1200 as of today and don't appear to have be nearing an inflection point. We should know soon I guess...
I'm thinking worst case we build 3x as many hospitals as we have now, and make sure we can accommodate anyone who needs intensive care.
Not a useful short term solution but I don't see why not for the long term. It just becomes another infliction that we prepare for and handle the best we can.
Buildings can be constructed, beds and associated equipment and I did mean beds as in hospital beds with associated equipment (ICU or otherwise) - where are you going to educated and train doctors and nurses to manage 3X.
Also, a common argument would be 3X is for such black swan events. What will happen to those beds, hospitals and manpower in a normal situation, especially with costs associated with educating and training medical professionals.
Don't get me wrong, I'm onboard with the fact that something fundamentally needs to change all over the world.
>where are you going to educated and train doctors and nurses to manage 3X
I suggest introducing a medical equivalent of military reserve forces/organized militias. These would be volunteers who train several times a year with medical professionals, to be called up in emergencies. Training would be limited to the skills most important in a pandemic. To incentivize volunteering, they could be given priority for medical treatment when resources are limited.
Even so, if those volunteers who are going to be performing dangerous and invasive (but potentially life-saving) procedures (like intubating people) and making snap life-or-death decisions (that require aptitude + years of medical education + experience, to avoid inadvertently killing their patients), we're going to need to have a very different set of expectations about these emergency volunteer medics/nurses than we would have for professional medics/nurses. With respect to death rates, expertise, errors, negligence, professional standards, how they will respond psychologically to the work. They would probably be better than nothing, but I imagine that an average person would rather have professional treating them than a volunteer, so that would be something that we would have to work through as a society.
With the economy strangled, how would it be possible to build more hospitals. At some point you can't ask people that don't want to do it to work for free.
On the bright side, that new way of life could help reduce the rate of climate change if it means fewer international flights, more local production of goods, the collapse of the cruise industry, etc.
The other possibility that few want to talk about is ADE, antibody-dependent enhancement (ADE). ADE is a slim possibility, but it would be devastating if it is. Basically it's when the virus uses white blood cells, which are supposed to kill it, to replicate. HIV and Dengue uses ADE. MERS (a coronavirus) doesn't appear to use ADE, but the jury is out on SARS (another coronavirus).
It means that you can get reinfected and a vaccine is near impossible.
We won't know about ADE because of the strict lockdown conditions that are still going on in China. If we start seeing more and more reinfections when things are relaxed, then we're in trouble.
"We also generated monoclonal antibodies against SARS-CoV spike proteins and observed that most of them promoted SARS-CoV infection. Combined, our results suggest that antibodies against SARS-CoV spike proteins may trigger ADE effects. The data raise new questions regarding a potential SARS-CoV vaccine, while shedding light on mechanisms involved in SARS pathogenesis."
Can someone tell me if the virus could be persistent? The virus is related to chickenpox according to [0]. And according to [1] "Once chickenpox has resolved, the virus may remain inactive in nerve cells." Risk factors for shingles are: "Old age, poor immune function, having had chickenpox before 18 months of age".
Heard something about this on one of Sam Harris' two podcasts on the subject this week - that this is typically because of a false negative test (indicating recovery from the virus) during what in reality is a longer, uninterrupted period of infection.
Sam's conversation with Amesh was terrific. It's eerie to think of this extraordinarily disruptive event as a "dress rehearsal" for a similarly transmissible contagion with a much higher fatality rate.
There already are/have been contagions that are as or more transmissible (in terms of R0) with much higher fatality rates, like SARS, MERS, polio and smallpox. But its difficult for a disease to get widespread or sustain itself when its both highly transmissible and deadly, because it often is instantly noticeable when individuals are sick, when outbreaks occur, and so its easier to contain and it burns itself out quickly.
Please be crisp on this. That is one hypothesis, but do we have the data yet to make sure it is the answer? I'm doubtful. Could also be unknown recall rates on the test. Could be plenty of things.
I am just meaning to be clear and not to stretch claims beyond what we know.
So, for example, I have a hypothesis that this is mainly baseline lung damage causing severe cases. That said, I cannot claim that is what it is.
I'm sure I have been sloppy and pushed this idea some without being clear it is just a hypothesis of mine. That said, I try and be clear with that message.
The part of Italy hit also has air quality, per aqi searches, that is comparable to the region in China that was hit hard.
Have people looked that it is not age, but baseline damage to your lungs that is the main factor in serious cases? Older people will have more exposure to local air pollution, just from having lived longer. That existing damage can be what contributes to complications, right?
My understanding is PCR doesn't actually test for the virus itself. It tests for antibodies. Such that, once you get a virus and have antibodies, you have them for life. The idea of getting it twice seems odd.
No, PCR test for a given RNA or DNA block. It will detect the virus, it will detect dead viruses, it will detect neutralized viruses, and it will detect virus bits.
No, PCR is not an antibody test. It amplifies DNA or RNA sequences which are known to exist in the virus. If enough unique sequences are found the test is positive.
> it doesn't actually test for the virus. It tests for DNA / RNA presence
The virus is nothing but DNA or RNA.
The snippet testing establishes a statistical baseline that rules in the presence of the specific dna/rna of the virus to within the required certainty.
In other words, you don't have to feel every inch of an elephant to know for sure you've got a hold of one. Just enough features to make it unique to just elephants.
If you can get reinfected, there's a good chance that the second infection will have a particularly high mortality rate, because this virus likely has a property known as antibody dependent enhancement[1]. Long story short, your normally protective antibodies actually work for the infection. This was a property of past coronaviruses like SARS and is likely why no vaccine was successfully developed.
Well, not exactly, it means that "immunity" may actually be dangerous or fatal. Because immunity implies release of antibodies on re-exposure, except in this case the antibodies bind to the virus, as normal, but then the virus infects much more readily, prompting the body to produce more antibodies and mount an ever greater immune response in a dangerous cycle.
The false positive rate is nowhere near 80%. All positive test results - both false and true - are at less than 5%.
80% might be the probability that an asymptomatic patient who tests positive is actually clear, but that's not what the statistic "false positive rate" means.
The term "false positive" is the one used in the NIH-linked article:
"Potential false-positive rate among the 'asymptomatic infected individuals' in close contacts of COVID-19 patients"
https://www.ncbi.nlm.nih.gov/pubmed/32133832
This isn't an NIH-affiliated article, to be clear. It's from a Chinese set of authors on a Chinese journal. But, it's not, because the article is now nonexistent.
There's a possibility for false-positives. I think there's a type of test that looks for an enzyme that you could have without contracting the virus.
I saw an article in HN this morning, but I can't find it anymore.
Also, false positives could happen as a result of bad logistics and management of the specimens.
Some useful sources that seem to validate the occurrence of false positives:
- This research on testing specifically calls out the fact that their method didn't yield false positives in trials: https://www.eurosurveillance.org/content/10.2807/1560-7917.E..., which seems to indicate that it's common for false positives to occur when developing testing methods for new viruses.
- This research talks about false positives in asymptomatic patients: https://www.ncbi.nlm.nih.gov/pubmed/32133832. "In the close contacts of COVID-19 patients, nearly half or even more of the 'asymptomatic infected individuals' reported in the active nucleic acid test screening might be false positives."
The tests are not accurate. [1] We are running around like chickens freaking out about tests. The only thing to do at this point is Social Distancing so the growth curve flattens out. Testing is NOT a solution. Testing will not make a sick person better. We have limited resources. Testing is being advocated by those trying to trace the community spread. I have news for you, if you think you have it you got it! Everyone will get it. Tracking this is a waste of resources at this point as the false positives mean additional limited Frontline Health Care workers treating actually sick individuals. We need to minimize the community spread, that means stay away from events. Work from home.
Individuals should self quarantine at any sign of illness. Critical patients should be admitted to hospitals. Everyone else should do everything in their power to slow the spread. You got a cough? Stay home. You feel tired or run down? Stay home. You have a fever and it went away? Stay home for the next 14 days. If your employer will not let you work from home, email them that you believe you are an asymptotic carrier of the COVID-19 virus and if they will not let you take paid sick leave or work from home you will be in the office immediately. Tell all your coworkers you requested to stay home and management wouldn't let you... Let the lawyers sort it out with HR.
"Testing is NOT a solution. Testing will not make a sick person better. ... Tracking this is a waste of resources"
This is just wrong on so many levels.
First, on an individual level, if doctors know you're infected with COVID-19, and your illness is severe enough, they might be willing to try an experimental treatment (like chloroquine) that they wouldn't for seasonal influenza or some other illness.
You might also be offered to participate in one of the hundreds of research studies that are ongoing in trying to find a treatment for this disease. You would not be a candidate for those studies unless they knew that you did in fact have COVID-19.
If doctors know you are infected with COVID-19, they are also more likely to isolate you and wear protective equipment that is essential to keep the disease from spreading to our precious medical personnel and vulnerable hospital populations.
Then, on the public health level, we need to understand how this disease is spreading, who is the most vulnerable and who is the least vulnerable and why. We also need to understand who has recovered and why they've done so, and if people have gotten sick again from re-infection, and why. Alternatively, maybe people have had been re-exposed to the disease but not gotten sick. Why is that?
We need to effectively plan for future outbreaks, to allocate precious resources to places that are the most affected, to quarantine areas that are hardest hit.
None of that can be done unless we have a better grasp on who has the disease and who doesn't.
Testing is critically important for all of this and more.
To advocate for the abandonment of testing simply because it's not perfect is madness. It's better to drive with one eye open than both eyes closed.
--edited because I don't think it matters if there are false positives what matters is the public understands the serious nature of the situation.
I have no medical training but below is my observation
Your points are valid (not regarding false positive rates), but the population still thinks the numbers put out are valid. So if we could ramp up testing very quickly (which seems to be possible given what the Cleveland Clinic is able to do) it would be beneficial for the public to see how bad the situation is. I haven't been able to convince anyone with symptoms that they are in fact likely to have it. (it could also be useful for hospitals to apply specific treatment regimens, when they get more defined)
Extensive testing is very useful at the beginning. It becomes less useful as the pandemic progresses.
A danger is that so much outrage has built up over the US’s failure to test that lobbying for testing will result in too many resources devoted to testing long after it’s still useful.
Ignoring the controversial parts of your comment - voluntary distancing to the point of "work disobedience" is of extreme importance, and we developers should responsibly lead the charge and flat out stay home regardless any policy or management opinion.
We have it easy we can trivially work from home and no one will fire us during this crisis. So don't wait just do it.
There are many businesses out there that are going to be suffering heavily from the total collapse of tourism, downtown office work, community events, etc; I wouldn’t assume any job is sacrosanct given that level of belt tightening.
Work from home. This is great advice for people who work by typing commands on a computer. Seems like people who are in tech think that coding, chatting on slack, etc. is what work is all about. There are so many jobs out there that we depend on require that people physically come to work.
I wonder what percent of jobs are reasonably safe to do (e.g. no forced close proximity to others). Office jobs are particularly bad and often easy to do from home, and many warehouse jobs don't have as close of proximity to other workers (many machines are operated by individuals), while jobs like trucking require almost none.
>I have news for you, if you think you have it you got it! Everyone will get it. Tracking this is a waste of resources at this point as the false positives mean additional limited Frontline Health Care workers treating actually sick individuals.
I'm glad to see someone say this. The over reaction is causing more problems than the actual virus. With every other recent potential pandemic, there was a reasonable response, the severity of the diseases were responded to accordingly, panic was at a minimum, especially considering more recent scares have been with viruses that cause far more serious diseases than this latest one.
This time, there's been an extreme focus on infection rates and zero focus on actual symptoms, which from every account i've seen so far, do not seem to be very terrifying for 99% of the population, yet the reaction has been just over the top everywhere.
This is going to spread around the world, we'll either get it or we won't, it's not going anywhere, it's out in the world, as soon as the first person got sick and spread it, it was inevitable. There's so much effort globally going into trying to stop or hide from this and I still don't really understand why.
When I was a kid, it was a regular thing to expose kids to chickenpox because it was just better to get it and get it over with, chickenpox sucked a whole lot. A whole lot more than having covid-19 would be from what I can tell.
It's the symptoms of a disease that scare me, not whether i'll get it. Personally, I was a lot more worried about the recent flu virus from a few years back that was killing young healthy people, than this disease that's not much more than a bad cold unless you're knocking on death's door already or in your 80's.
If people that get it, don't even realize they have it and nothing bad is really happening to them, then why should I be losing my shit and freaking out? Why should I be scared of getting a disease that's about the same as something I get nearly every year anyway?
> do not seem to be very terrifying for 99% of the population
This is a dangerously bad take. The death rate is in the 2-3% range. Hospitalization in China was 15%, with 5% in critical care.
Even if you are not personally vulnerable, please understand that those who are also actual humans, and have actual humans as family members. And if you can't manage to care about that, recognize that a pandemic of this magnitude could easily overwhelm the US hospital system: https://www.statnews.com/2020/03/10/simple-math-alarming-ans...
As we're seeing in Italy, an overwhelmed hospital system leads to increase death rates from many other causes, because suddenly the level of care goes down. If all the ICU beds are full and you, say, get hit by a truck, you'll be triaged along with all the other people needing ICU. If a COVID-19 patient looks more likely to recover than you, well, you'll be left out in the hallway.
The disease is not bad for most people. HOWEVER, the the real threat is too many people getting it at once, 10% need critical care, and that overloads our medical services.
Because you aren't everyone else. There are lots of people that would be hit very hard and require intense hospitalization or face death if they were to get COVID-19.
Furthermore, this would put a strain on medical resources if the number of patients is higher than medical capacity. Suddenly all the treatable conditions that require medical supervision become deadly because there aren't enough medical personnel and resources to treat everyone. Got in an accident requiring emergency care? Maybe you won't be able to get it now.
More still, all the medical personnel who would otherwise have gotten a flu shot and been immune to its spread now have to worry about catching COVID-19 and having medical resources spread even more thin, at the worst time.
You can't just think of yourself, you have an ethical duty to consider the externalities of your actions.
Edit: Maybe I should point out that panicking or worrying about it does no good and that should be minimized as much as possible. However, if people are not treating it as seriously as they should, then maybe a little bit of panic and worry would be a good thing to get people into a proper state of mind about what is going to happen.
Well one concerning statistic is the 20% of cases that require hospitalization. Not sure what that is for the standard flu but I suspect its not that high. If the hospitals are full like what happened in Italy and China and people who need medical help can't get it, it seems like the death rate is much higher like 3.5% vs. .1% for the standard flu. The virus really is mostly a danger for the elderly and so the public health goals are slowing the spread, flattening the curve so that the people who get it whose immune systems aren't able to overcome it as well can get the medical help that they need vs. being told to go home and die like they have had to do in Northern Italy.
Also the difference in asymptomatic incubation is a lot higher than the flu so people can spread it w/o realizing it. I read flu has max of 4 days incubation with typical period of 1.5 whereas this has a mean of 5 and max of 14, and possible shedding during asymptomatic period so you could be infecting people a lot longer before you get sick and its harder to trace all contacts.
I think you're slightly off track as to the frustration with lack of testing:
Let's start with widespread complacency opposed to requests to take distancing measures: people (not me, but .. read FB comments from regular people on news stories) are mad at sports events being canceled because "nobody has the virus". So we don't get the social distancing response needed.
If on the other hand we had some testing data from the general population, or even from just mildly sick people, then the requests for social distancing could be presented with "and we know this thing is here now, so these measures are going to have a significant effect".
Every meaningful authority is suggesting you do the opposite — Do not panic, there is no need to freak out.
But you should still avoid getting it and spreading it to others. Having a slower, more controlled growth gives us significantly more time to find a vaccine and learn more about the virus.
People who are immunocompromised, whether by age or otherwise, are a vulnerable part of our society worth protecting.
This virus isn’t an inconvenience like the chickenpox, it is killing people.
This is what Illinois seems to be doing anyway. It makes sense to me. We don't have enough tests or medical staff to test everyone. Easier to just make everyone stay home.
"If you are sick and have respiratory symptoms, such as fever, cough, and shortness of breath, stay home unless you need medical attention"
http://dph.illinois.gov/topics-services/diseases-and-conditi...
This might be right, iff testing were some kind of binary choice that needed to be made one way or the other. But why should the tool of testing be politicized and debated, rather than it simply being one resource available to doctors to use as they see fit?
You do need testing to dial in what level of social distancing brings the rate down to a level the health care system can handle without dragging out the crisis needlessly long.
In fact, you won’t know if your test is inaccurate if you don’t test! Over and over again I hear people talk about how it is a waste of resources to test. Tests are not expensive in time or material. They will pay off.
No, they don’t help you cure anything. We dont have a cure!
Sure, you can randomly shotgun a bunch of potential solutions and hope for the best, but any systematic improvement process relies on quantitative measures and root cause analysis.
Random changes can be positive and you don't need to quantify anything to do them.
Also quantifying after the fact isn't what we're talking about so I could test and verify that indeed you did improved something 10 years ago and you made that improvement without quantifying anything yourself.
Too bad we don't have 1000 societies to randomly try things on.
Also you don't know that you rolled a six, the probability is high that you did, that's very different. If you don't know where you rolled the number you wanted, how can you repeat it? If you can't repeat it how can you build on top of that?
> Also you don't know that you rolled a six, the probability is high that you did, that's very different.
By that standard you don't know anything about the world at all - gravity may stop working the next minute - it's unlikely but not impossible. We don't have a proof it won't - we only have assumptions(models) supported by statistics. For me the standards that physics use is good enough - I say I know gravity works and I know I rolled a 6 when I rolled 1000 d6. You might call that differently but I'm pretty sure you won't jump out of a cliff and you won't bet money on NOT rolling a 6 in 1000 tries.
> Too bad we don't have 1000 societies to randomly try things on.
That's exactly why we shouldn't wait for results.
We have data from 1000s of people though and several countries that tried various strategies. Social isolation works best so we should do that, immediately.
With exponential growth doing the right thing NOW is more important than making sure you're doing it in an optimal way but a week later.
> If you don't know where you rolled the number you wanted, how can you repeat it? If you can't repeat it how can you build on top of that?
In the case of this disease we know how to prevent it overwhelming our healthcare systems so that less than 1% of population dies instead of over 5%. That's the most important thing, producing the vaccine and drugs, calculating the exact number of people sick, discovering the exact properties of the sickness - these things come after the fact. We won't have a vaccine nor drugs in time anyway.
People arguing to measure and then act in case of a disease that infects 1000 times more people every month are insane. In 3 months the whole world population would be sick and most of it AT ONCE. Who will treat the 5-10% of patients that need help? Nobody - that's who. So they will die.
Testing and understanding the past is not the same as predicting the future. Our physical world has been extensively tested, which how we learned about it. If you want to treat gravity stopping in the future as a probability you can, but once but the more you understand the more you would realize that it is astronomically low.
This is not the same as saying that from some technical extreme semantic definition that something can be improved without testing results. In a complex system you need to know your results to inform your path forward. Trying to come up with some super narrow, reductive, irrelevant definition on your own is worthless in this context.
{kind=link}
1. Is it possible to get COVID-19 twice?
2. If (1) is true, are the symptoms the same (if applicable)?
3. If (1) is true are you still contagious?
4. There's evidence that there are multiple strains, can you get both strains?
5. What's the likelihood that a mutation will occur once treatment is more widespread?
6. Does the heat make it significantly less likely for you to get COVID-19?
My impression so far is that we'll never get rid of this thing, and at best this will be something like the seasonal flu, where we'll just have to live with it and great shots yearly.